fetching data ... 
Background: Systemic sclerosis (SSc) is characterized by progressive fibrosis and microvascular dysfunction that involves multiple organ systems, including kidneys. Kidney involvement, beyond the scleroderma renal crisis (SRC), is often asymptomatic and underdiagnosed, associated with subclinical renal vasculopathy characterized by abnormalities in renal microcirculation and mild changes of glomerular filtration rate (GFR). Kidney involvement is rare in isolated Sjögren’s syndrome (SS) and reported between 5% and 14% in european patients and approximately 30% in asian patients.
Objectives: The aim of the study was to assess renal involvement in SSc and SS and follow its progression over a three-year period.
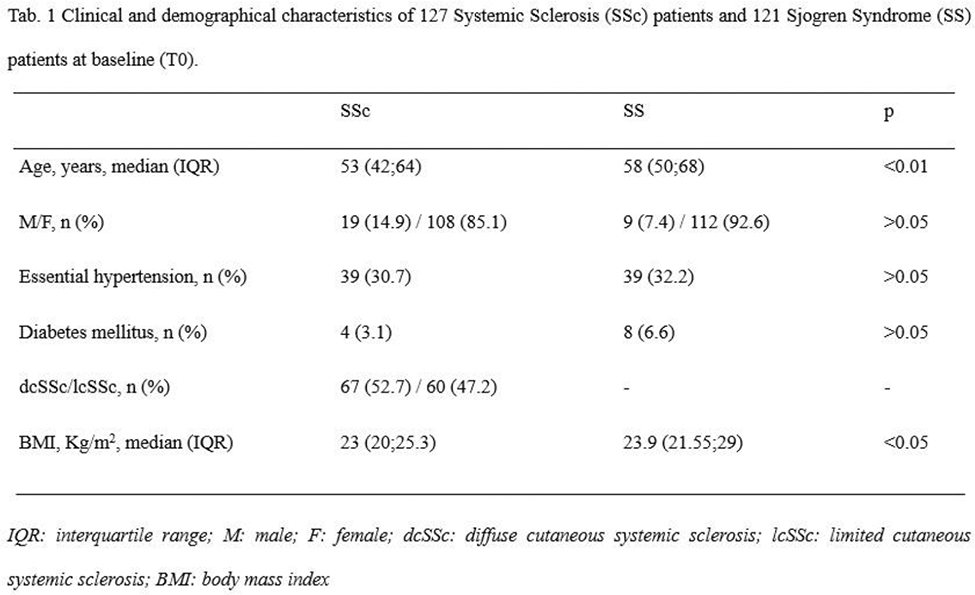
Methods: Patients with SSc (2013 EULAR criteria) and isolated SS (2016 ACR/EULAR criteria) were consecutively enrolled. Demographic and clinical characteristics at baseline (T0) were gathered including sex, age, body mass index (BMI), history of essential hypertension and diabetes, serum creatinine, and estimated GFR calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. Exclusion criteria were presence of SRC, atherosclerosis renal artery stenosis and other secondary causes of hypertension, glomerulonephritis, urinary tract obstruction, urinary infections, heart failure, pulmonary arterial hypertension, malignancies. All patients were followed for three years (T1) with renal function assessment. Group comparisons were made using the Student’s t-test or Mann-Whitney test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. A significance level of p<0.05 was considered.
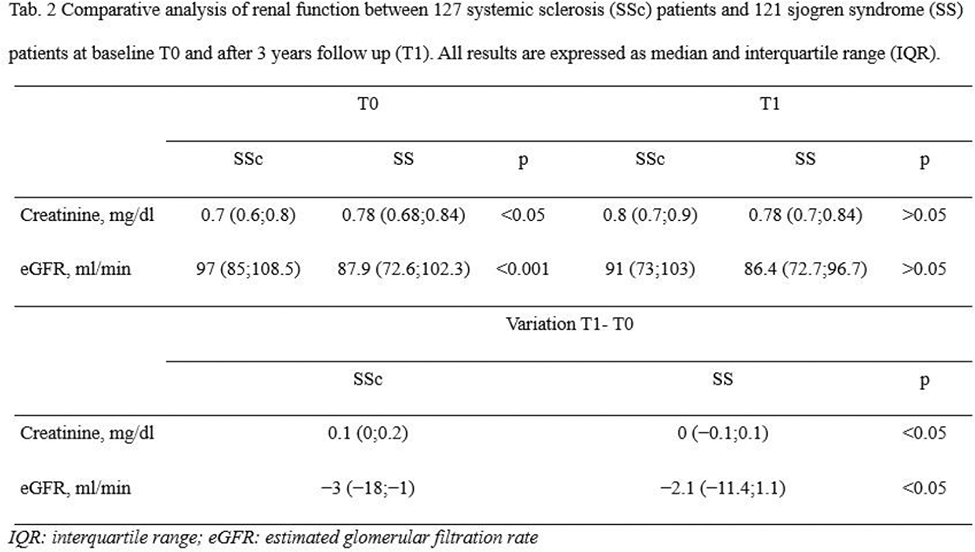
Results: A total of 248 patients were enrolled, 127 SSc and 121 SS patients. Their features at baseline (T0) are summarized in Table 1. Table 2 summarizes the comparative analysis of renal function between SSc and SS patients at baseline and after 3 years. SS patients had similar median serum creatinine both at T0 and at T1 [0.78 mg/dl (IQR 0.68;0.84) vs 0.78 mg/dl (IQR 0.7;0.84), p>0.05], but a higher eGFR at T0 than at T1 [87.9 ml/min (IQR 72.6;102.3) vs 86.4 ml/min (IQR 72.7;96.7), p<0.05], with a variation of −2.1 ml/min (IQR −11.4;1.1). SSc patients had a statistically significant lower median serum creatinine at T0 than at T1 [0.7 mg/dl (IQR 0.6;0.8) vs 0.8 mg/dl (IQR 0.7;0.9), p<0.001], with a variation of 0.1 mg/dl (IQR 0;0.2), and a statistically significant higher median eGFR at T0 than at T1 [97 ml/min (IQR 85;108.5) vs 91 ml/min (IQR 73;103), p<0.001], with a variation of −3 ml/min (IQR −18;−1). In both SSc and SS eGFR median variation was statistically significant higher in patients affected by systemic arterial hypertension compared to those without [−12.2 ml/min (IQR −16.32;5.42) vs −1.8 ml/min (IQR −3;0.4), p<0.01 for SS patients and −18 ml/min (IQR −26; −12) vs −2 ml/min (IQR −7;2.25), p<0.001 for SSc].SSc patients had a significantly higher variation compared to SS patients both for median serum creatinine [0.1 mg/dl (IQR 0;0.2) vs 0 mg/dl (IQR −0.1;0.1), p<0.05] and median eGFR [−3 ml/min (IQR −18;−1) vs −2.1 ml/min (IQR −11.4;1.1), p<0.05].
Conclusion: In both SSc and SS patients, renal involvement exhibited a subclinical pattern (eGFR > 60 ml/min). This preliminary study also highlights slight differences in renal involvement and its progression between the two groups considered. In SSc patients, creatinine levels at T0 are, on average, lower than in pSS patients possibly linked to their reduced muscle mass. Over time, SSc patients tend to show a tendency toward eGFR reduction, for the continuous microvascular damage leading to chronic hypoxic-ischemic injury.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.