fetching data ... 
: The shape of the spine is critical in maintaining posture on the vertical axis, and the morphology of the pelvis affects the distribution and dynamics of mechanical stress along the spine. Pelvis and spine angulations, called spinopelvic parameters, vary individually, hence, the site of mechanical load in individuals. Particular types of spino-pelvic parameters are associated with different types of degenerative diseases. However, whether baseline pelvic parameters affect the location of new bone formation and the degree of radiographic damage in patients with SpA is not known. This study aimed to prospectively investigate the effect of pelvic parameters on syndesmophyte formation and radiographic damage in the spine in a heterogeneous group of SpA patients.
Methods: Radiographic SpA (r-SpA) patients currently under follow-up in the MARS (MARmara Spondyloarthritis) outpatient clinic were included. Two readers independently scored the radiographs according to the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS), and two readers calculated the spinopelvic parameters. The average scores were used. The relationship between pelvic parameters and radiographic progression was investigated using logistic regression analyses adjusted for potential confounders. Interactions were tested.
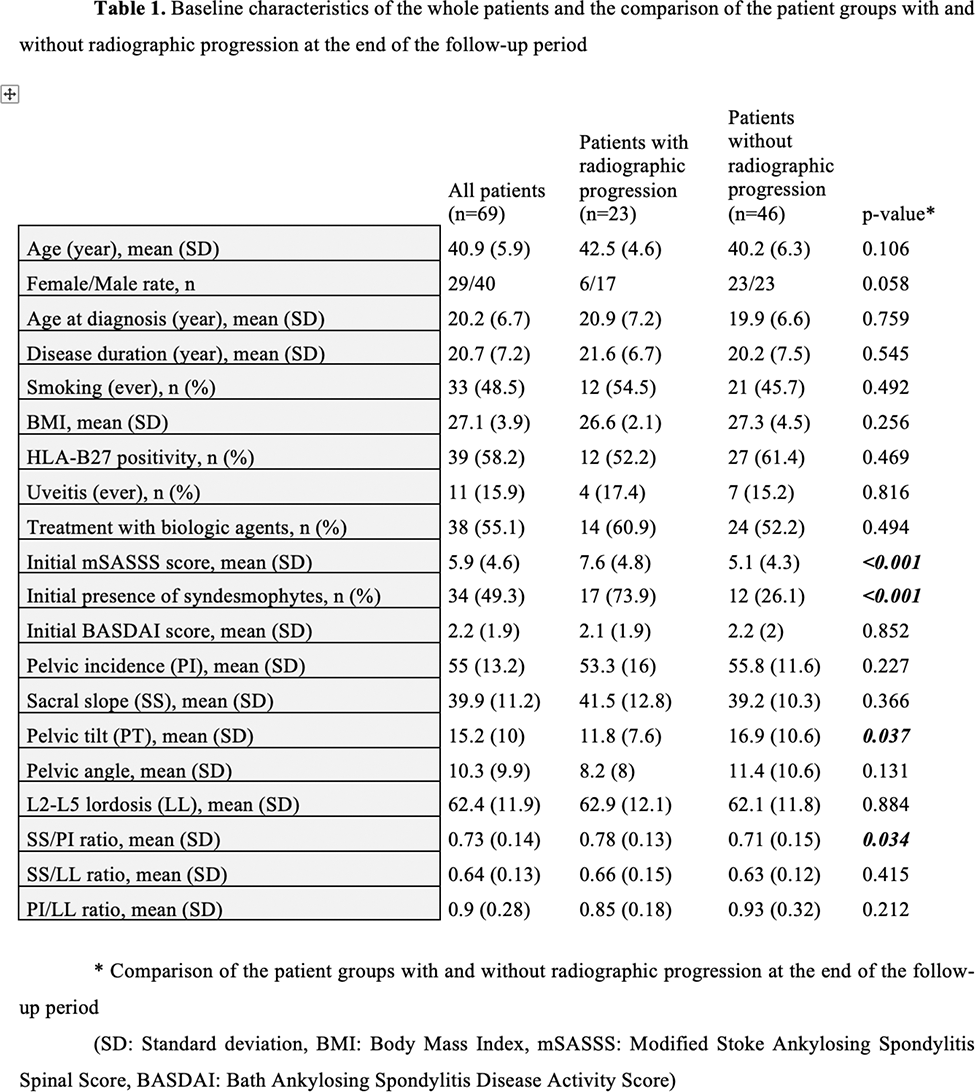
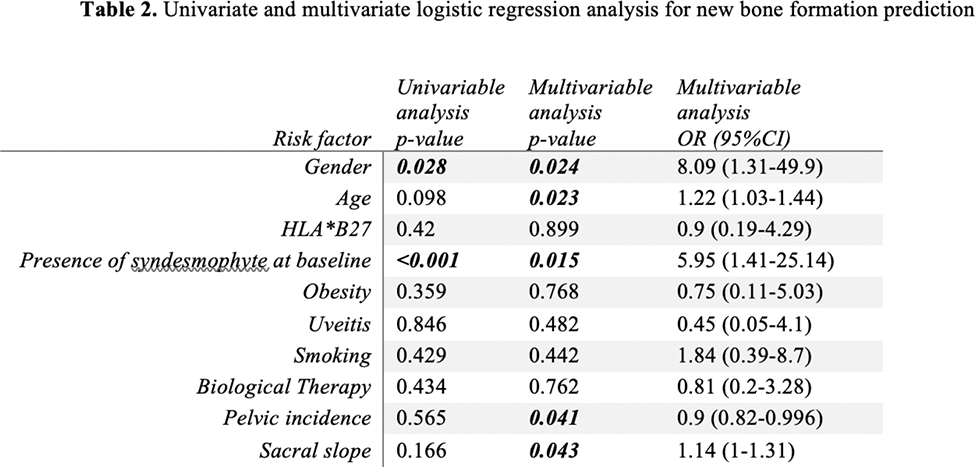
Results: Sixty-nine patients completed the prospective follow-up period, with a median (IQR 25-75) follow-up period of 47.7 (34.6-52.8) months. Of these patients, 40 (58%) were male, and 39/68 (58.2%) were HLA*B27 positive, 38 (55.1%) were under treatment with biological therapies during the follow-up period. Radiographic progression developed in 23 (33.3%) of 69 patients. The mean (SD) mSASSS and the mean (SD) the number of syndesmophytes of these patients, respectively: at the time of enrolment were: 8.5 (4.6), 2.1 (1.8); after two years of follow-up were: 11.1 (4.28), 2.6 (1.9); at the end of the study were: 14.5 (4.7), 5 (2.7). Patients with radiographic progression statistically significantly had a higher baseline mSASSS (p<0.001), syndesmophyte count (p<0.001), PT measurement (p=0.037), and SS/PI (p=0.034) ratio than those without. No statistically significant difference existed between those with and without radiographic progression in gender, smoking, BMI, HLA*B27 positivity, and receiving biological treatment rates (Table 1). When PI, SS, and LL, were compared, PI was lower, and SS was higher in those with radiographic progression than those without. However, the difference between both parameters did not reach statistical significance. Nevertheless, the SS/PI ratio was statistically significantly higher in those with radiographic progression (in groups with and without radiographic progression, respectively; mean (SD): 0.78 (0.13) and 0.71 (0.15); p=0.034). Multivariate logistic regression analysis revealed that SS with an OR of 1.14 (95%CI: 1-1.31 p=0.043) and PI with an OR of 0.9 (95%CI: 0.82-0.996, p=0.041) were significant risk factors that are independent of the effects of previously reported risk factors or new bone formation.
Conclusion: The SS/PI ratio is significantly higher in patients with radiographic progression. The baseline SS/PI ratio is correlated with the progression of mSASSS per unit time under follow-up, and the PI itself has a negative correlation with the progression in the lumbar spine. These correlations are more emphasized in the male sex and increase with age. In this model of new bone formation, information on HLA*B27, obesity, uveitis, smoking, and treatment had no additional contribution.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.