fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that affects multiple organs, including the kidneys, leading to lupus nephritis (LN) in 40-75% of patients. Lupus nephritis (LN) is a severe manifestation of SLE with substantial clinical and prognostic implications. 1 However, there is conflicting data regarding the prognostic implications associated with the timing of nephritis onset. 2,3
Objectives: The study aims to explore the clinical characteristics and outcomes of LN patients with “initial” and “late onset”. Additionally, it compares the features of patients who had one or more instances of disease relapse with those who did not experience any relapse.
Methods: The study involved 243 patients diagnosed with SLE between 1970 and 2019 at our Lupus Clinic. Patients with renal involvement were categorized into two groups: “initial onset”, with renal issues at the disease’s start, and “late onset” developing renal involvement later. Demographic, laboratory, histological, and therapeutic data were collected for both groups. Categorical variables were reported as proportion and/or percentage, continuous variables were expressed as mean (±standard deviation) values. Continuous variables were compared using one-way Anova or Mann-Whitney test, categorical variables with Chi-Squared or Fisher’s exact test. P values <0.05 were considered statistically significant.
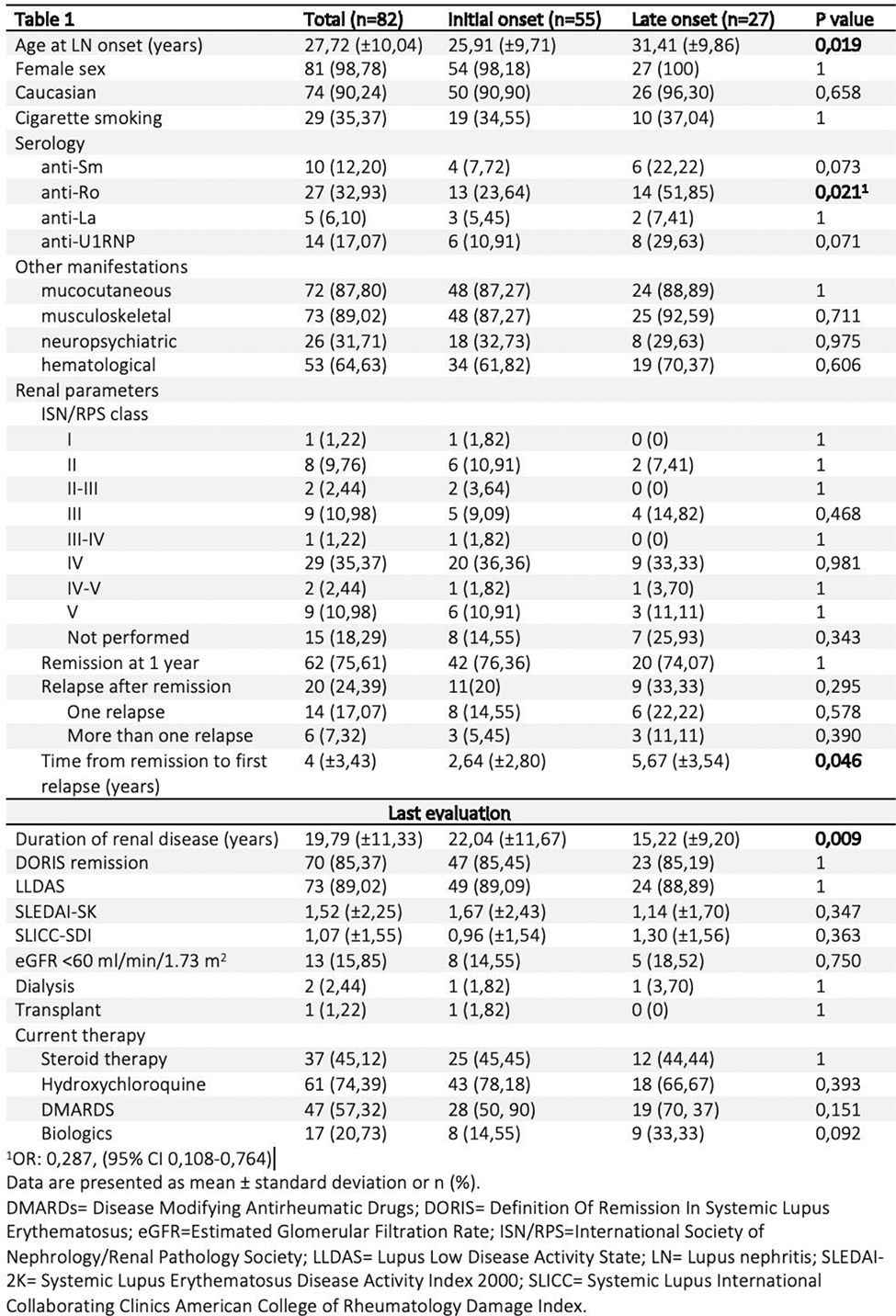
Results: Of these 243 SLE patients, 82 (33.74%) had renal involvement, mostly females (98.78%) and Caucasian (90.24%). The average duration of LN was 19.79 years (±11.33). At the last evaluation, 85.37% were in remission according to DORIS, 15.35% had eGFR < 60 ml/min/1.73 m 2 , 2.44% were on dialysis, and 1.22% underwent transplantation.
Regarding the timing of renal onset, 55 (67.07%) had an “initial onset”, while 27 (32.92%) had a “late onset”, with an average time from SLE onset to renal involvement of 5.73 years (±6). Differences were noted in age at renal disease onset, with “late onset” patients being older, and “initial onset” patients having a longer duration of renal disease (Table 1). No other significant differences were found in demographic, clinical, histological, and laboratory data, except for a higher frequency of anti-Ro antibodies in the “late onset” group (p=0,021).
Remission rates within a year and recurrence rates did not significantly differ, but the time until recurrences occurred was significantly longer for the “late onset” group (p=0,046).
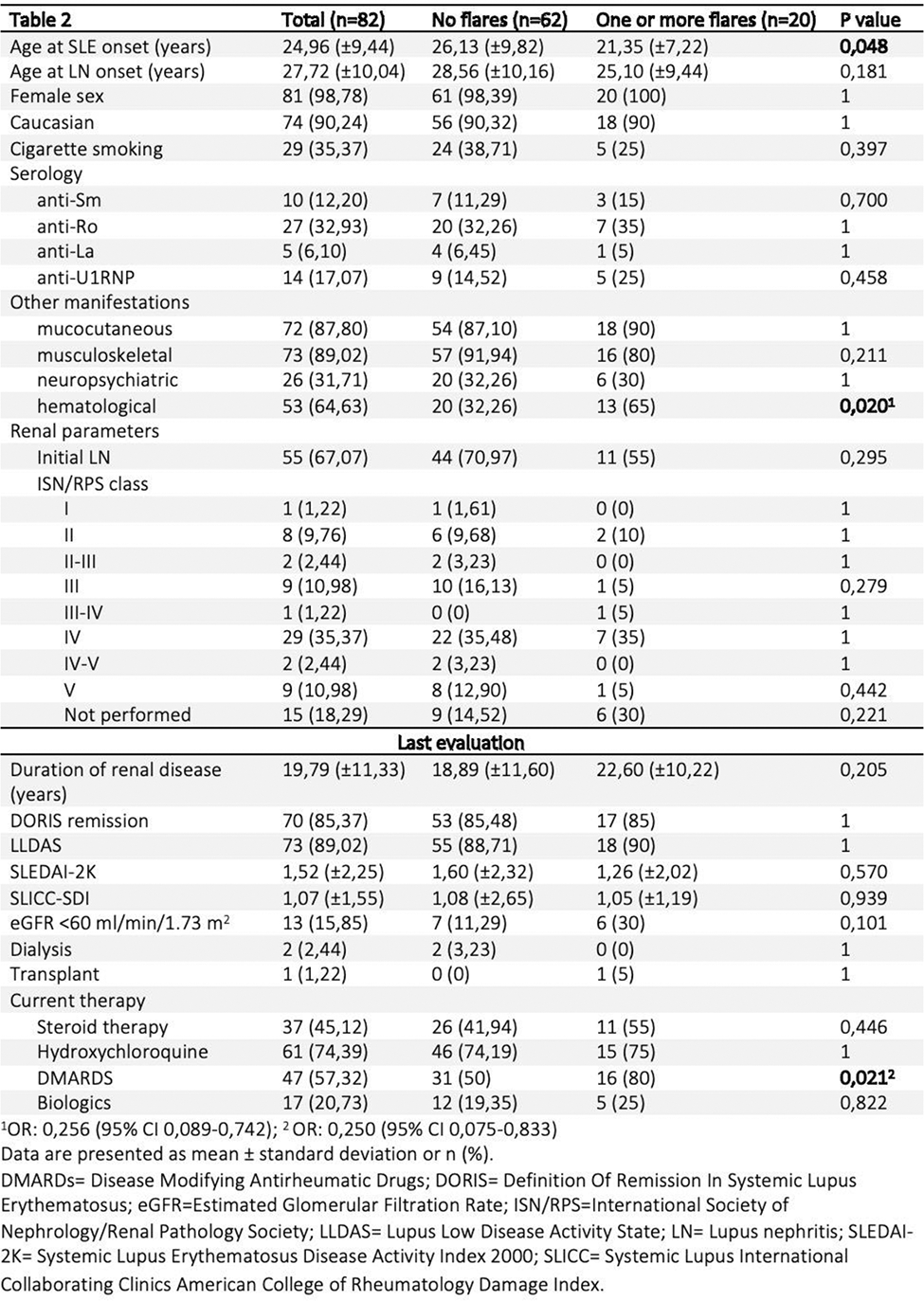
Comparing patients with renal disease exacerbations and those without renal flares, the former group was younger at SLE onset (p=0,048) and exhibited more hematological manifestations. No differences were observed in renal function, disease activity (SLEDAI-2K), or organ damage (SLICC-SDI). However, there was a notable distinction in maintenance therapy, with a greater use of disease-modifying antirheumatic drugs (DMARDS) in patients experiencing one or more disease flares (p=0.021).
Conclusion: The preliminary results confirm that renal onset typically occurs in most SLE patients at the disease onset. Patients with “late onset” exhibit a higher age at the onset of renal disease but a shorter duration of renal disease compared to those with “initial onset”. No differences were found in terms of disease relapses or the percentage of patients with chronic kidney disease. However, the “late onset” group shows a significantly longer time from remission to relapses, indicating a possible favorable prognostic factor for kidney disease in this subgroup. On the other hand, patients with one or more renal flares appear to have a more challenging-to-control systemic disease, leading to a higher frequency of long-term treatment with immunosuppressive drugs. Despite this, no significant differences were found in the prevalence of irreversible renal impairment. These results are preliminary and require confirmation by integrating data from the entire cohort of SLE patients followed at our center.
REFERENCES: [1] Lisnevkaia et al. Lancet. 2014
[2] Suzuki et al. IJR. 2021
[3] Oh Chan Know, et al. YMJ. 2020
Acknowledgements: NIL.
Disclosure of Interests: None declared.