fetching data ... 
Background: Lupus nephritis (LN), a major involvement of systemic lupus erythematosus (SLE), impacts up to 60% of SLE patients throughout their lives, with a progression rate to end-stage kidney disease ranging from 4.3% to 10.1%.
Objectives: This study aims to 1) assess the attainment of lupus low disease activity state (LLDAS) and remission in SLE patients with LN at a single center and 2) analyze predictors of LLDAS, remission, and stage ≥3 chronic kidney disease (CKD).
Methods: This retrospective, observational study included SLE patients diagnosed since 1977 with documented renal involvement via kidney biopsy. Demographic, clinical, and laboratory data were collected from the onset of renal disease to the last outpatient visit. CKD was defined as eGFR (calculated using CDK-EPI formula) ≤60 mL/min/m2, while LLDAS and REM definitions were based on criteria by Franklyn K. et al (Ann. Rheum. Dis., 2016) and van Vollenhoven RF (Lupus Sci. Med., 2021).
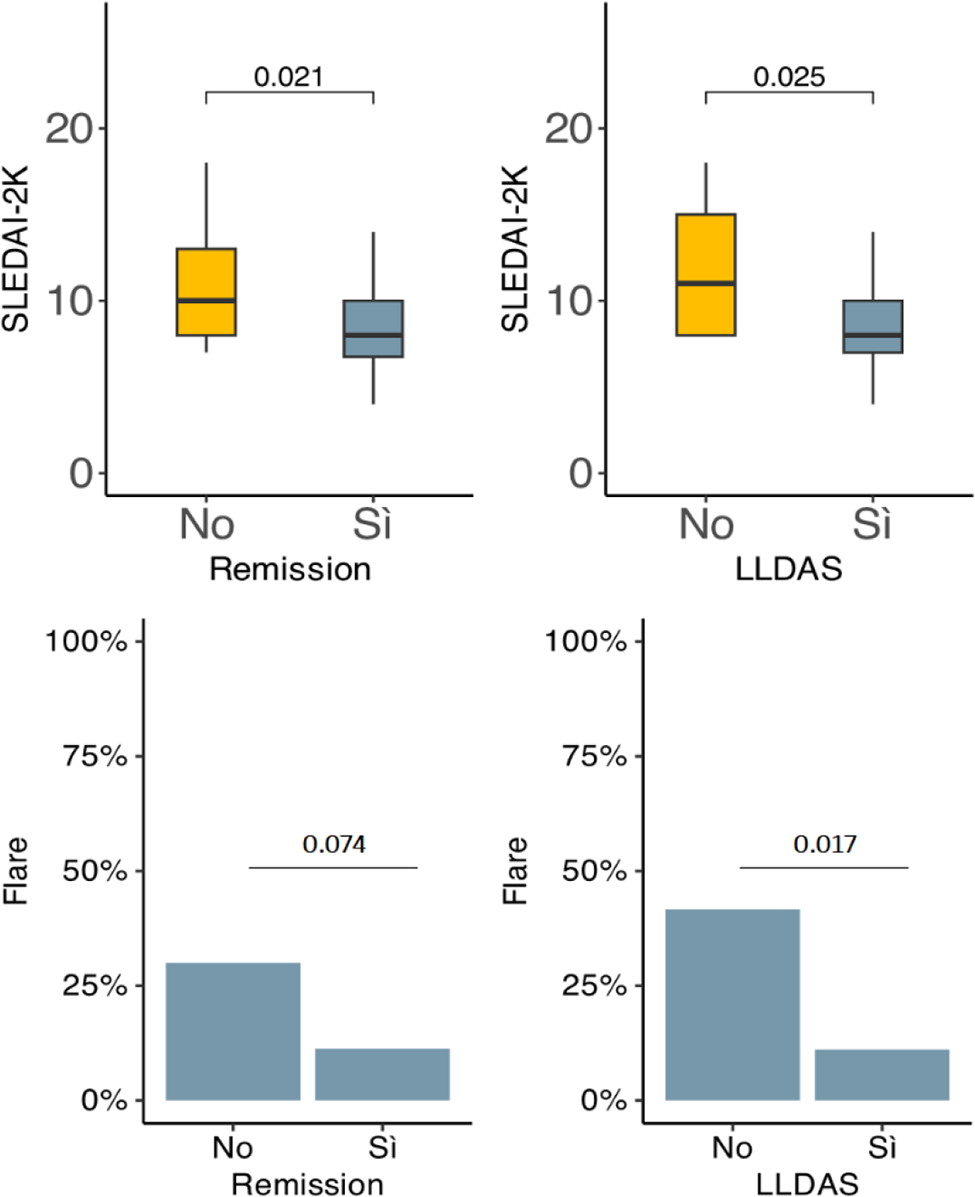
Results: The study comprised 87 patients, with 42 having proliferative glomerulonephritis (see Table 1). During the follow-up, clinical remission was achieved in 63 out of 83 (75.9%) patients, and LLDAS in 73 out of 85 (85.9%) patients, with an average time of 8.46 (±8.67) and 8.33 (±8.96) months between biopsy diagnosis and achieving remission and LLDAS, respectively. Univariate analysis indicated a statistically significant association between higher SLEDAI-2K and failure to achieve LLDAS (OR 0.88, p 0.049). The occurrence of at least one LN flare during follow-up was associated with a lower probability of achieving LLDAS (OR 0.17, p 0.01) but not remission (OR 0.29, p 0.05). Predictors of stage ≥3 CKD included a longer time between LN diagnosis and LLDAS/REM achievement (OR 1.08, p 0.02/OR 1.09, p 0.01), a higher SDI score (OR 1.82, p 0.02), and the protective effect of hydroxychloroquine use (OR 0.26, p 0.02).
Conclusion: In our cohort, higher SLEDAI-2K scores and the occurrence of LN flares were associated with a lower probability of response to therapy. A higher SDI score and a prolonged time to achieve REM/LLDAS serve as potential indicators of kidney function deterioration.
REFERENCES: [1] Gasparrotto M et al (Rheumatology Oxford, 2020), Franklyn K. et al (Ann. Rheum. Dis., 2016), van Vollenhoven RF (Lupus Sci.Med.,2021).
| Baseline characteristics (at histological diagnosis) | Total
| Proliferative
| Membranous
|
|---|---|---|---|
| Female, n (%) | 82 (94) | 38 (90) | 20 (100) |
| Age, (mean ± DS) | 33 (13) | 30 (11) | 30 (11) |
| Disease duration (years),(mean ± DS) | 4.6 (8.0) | 3.6 (6.7) | 3.1 (6.8) |
| Ethnicity | |||
| Caucasian, n (%) | 82 (94) | 38 (90) | 19 (95) |
| Afroamerican, n (%) | 3 (3.4) | 2 (4.8) | 1 (5) |
| Other, n (%) | 2 (2.3) | 2 (4.8) | 0 |
| Weight (kg), (mean ± DS) | 67 (16) | 70 (18) | 67 (14) |
| Height (cm), (mean ± DS) | 164 (7) | 164 (8) | 164 (7) |
| Smoker, n (%) | 39 (46) | 17 (41) | 9 (45) |
| Creatinine (mg/dl) (mean ± DS) | 1.08 (1.07) | 1.10 (1.09) | 0.74 (0.19) |
| Nephrosic range proteinuria, n (%) | 10 (16) | 6 (21) | 1 (5) |
| Anti-dsDNA positivity, n (%) | 69 (80) | 38 (90) | 13 (65) |
| SLEDAI-2K score, (mean ± DS) | 9 (4) | 10 (5) | 8 (2) |
| SLICC-SDI score (mean ± DS) | 1(1) | 0 (1) | 0 (1 |
Acknowledgements: NIL.
Disclosure of Interests: None declared.