fetching data ... 
Background: ANCA-associated vasculitis (AAV) is a systemic disorder primarily affecting small blood vessels. While its classic manifestations involve the respiratory and renal systems, central nervous system (CNS) involvement is increasingly recognized. The diverse CNS manifestations can be as ischemic or hemorrhagic events, parenchymal inflammatory lesions, pachymeningitis, cranial involvement, or hypophysitis.
Objectives: To highlight and analyze the incidence and disease characteristics of the patients with AAV-CNS involvement.
Methods: Patients with vasculitides are prospectively recorded to a web-based system since 2014 at Hacettepe University Vasculitis Research Centre (HUVAC). This database is screened for this study. In total, 189 patients diagnosed with AAV were enrolled in this study. Clinical records, imaging studies, and laboratory data were reviewed to identify cases with CNS manifestations. Patients were evaluated for their demographic data, AAV type, organ involvement, prognostic variables, and characteristics of the neurological features. We specifically included neurological findings that were verified to be a direct result of AAV.
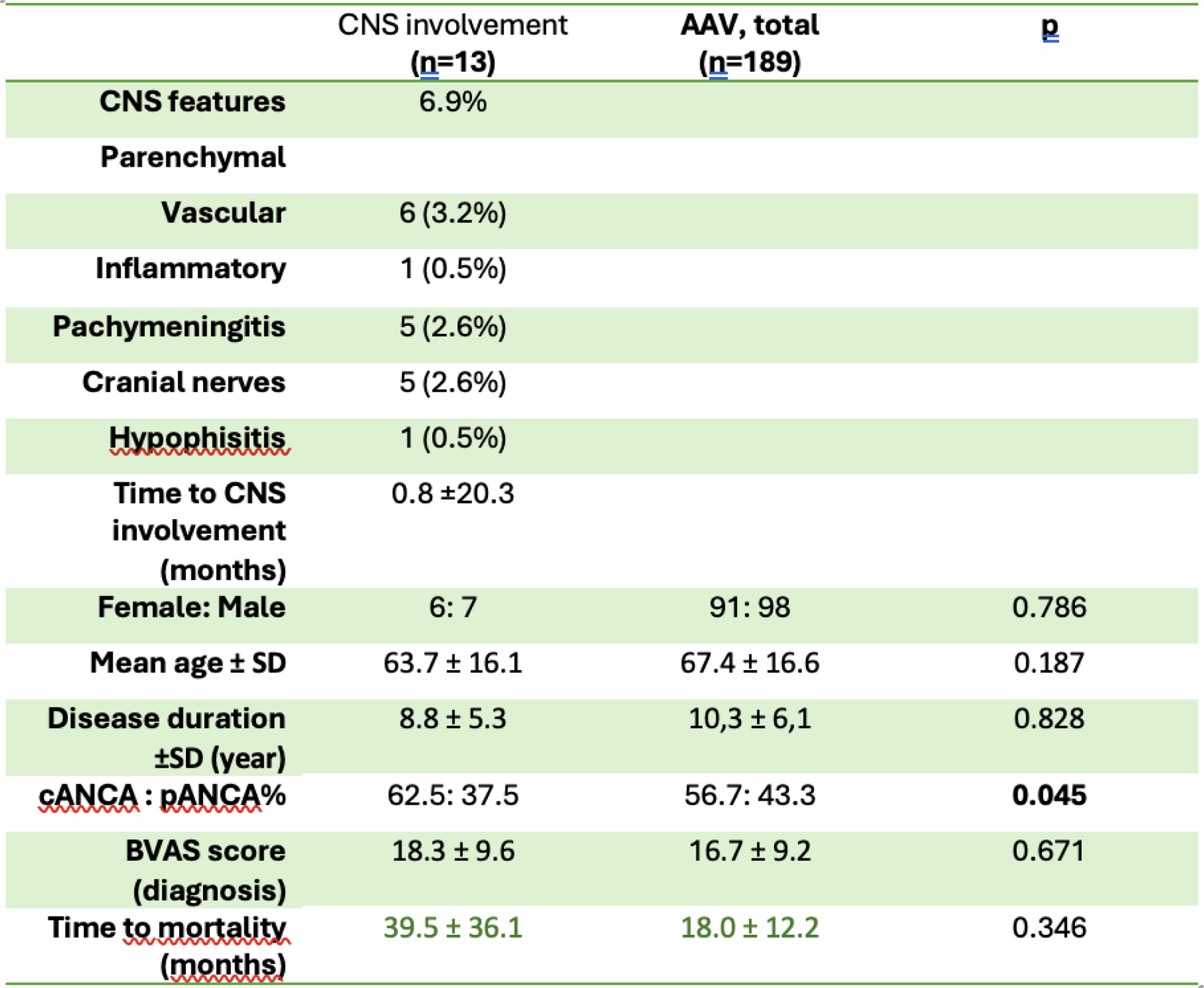
Results: Among the 189 patients diagnosed with ANCA-associated vasculitis (AAV), 13 individuals (6.9%) exhibited central nervous system (CNS) involvement, encompassing ischemic or hemorrhagic events (n=6), parenchymal inflammatory lesions (n=1), pachymeningitis (n=5), cranial involvement (n=5), or hypophysitis (n=1). Of these, 61.5% were male, with a mean age of 63.77 years (±16.07). 62,5 of the patients had GPA; 37,5 had MPA. The mean disease duration was 8.77 years (±5.31), and the diagnosis of CNS involvement occurred 0.77 months (±20.29) after the onset of the disease. When compared with the entire group, the CNS subgroup exhibited similar distributions in terms of patients’ sex, age, and disease duration. Notably, the CNS group had a slightly higher prevalence of GPA diagnosis compared to the overall group (p=0.045). Comparing the BVAS scores at the time of diagnosis, we observed similar values in both the CNS group and the overall AAV cohort (18.3 ± 9.6 and 16.7 ± 9.2, respectively; p=0.671).
In 76.9% of cases with CNS involvement, the diagnosis of AAV was established after the onset of CNS symptoms. Unfortunately, 15.4% of patients with CNS involvement succumbed to systemic complications or sepsis. Mortality ratios were statistically similar compared to the whole group (p=0.330). The average time to mortality after diagnosis was 18.00 ± 12.24 months in the whole group and 39.50 ± 36.06 months in the CNS group.
Notably, 38.5% of these individuals also exhibited peripheral nervous system involvement.
Three patients exhibited ischemic lesions, and another 3 had gliotic lesions, all of whom also presented with additional CNS involvement such as demyelinating lesions, cranial nerve involvement, or hemorrhagic lesions. Angiographic (MRA) evidence of vessel involvement was identified in 3 patients, 2 of whom had associated hemorrhagic lesions. Additionally, 1 patient with ischemic lesions displayed MRA abnormalities. Cranial nerve involvement was observed in 5 patients.
Hypertrophic pachymeningitis was present in 5 patients, and 2 of these individuals also had cranial nerve involvement attributed to a mass lesion in the soft tissues. Only one case involved a patient with a lesion in the hypophysis-hypothalamus region.
Conclusion: This study underscores the complexity of CNS involvement in AAV, revealing diverse manifestations ranging from vascular complications to inflammatory lesions, with implications for both diagnosis and patient outcomes.
The observed prevalence of CNS involvement in our study aligns with the lower range reported in the current literature. Notably, we exclusively included CNS cases definitively proven or directly related to AAV. Further exploration of these factors is essential for a comprehensive understanding of the spectrum of CNS manifestations in AAV.
Table 1.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.