fetching data ... 
Background: Timely diagnosis and treatment of systemic lupus erythematosus (SLE) are a current challenge. There is no consensus on the definition of delay nor a clear understanding of the associated factors, such as clinical, sociodemographic, cultural, and healthcare system characteristics.
Objectives: To develop a systematic review of quantitative studies focused on delay in diagnosis and treatment of adult patients with SLE, and to identify associated barriers and facilitators.
Methods: Electronic searches were conducted in Scopus, PubMed and Web of Science for studies published up to July 15th, 2023. Inclusion criteria were studies in adult patients that estimated delay in diagnosis and treatment and associated barriers and facilitators. The phases were: 1) consensus of eight expert rheumatologists on the keywords for an advanced query string search in the title, abstract and keywords; 2) titles and abstracts were screened by peer review; 3) the group reviewed full-text articles and filled a predesigned Excel format; 4) synthesis focused on identifying the variables related to delay in diagnosis and/or treatment; 5) the JBI Checklist for Analytical Cross-Sectional Studies [1] was used to assess quality with a maximum score of 8.
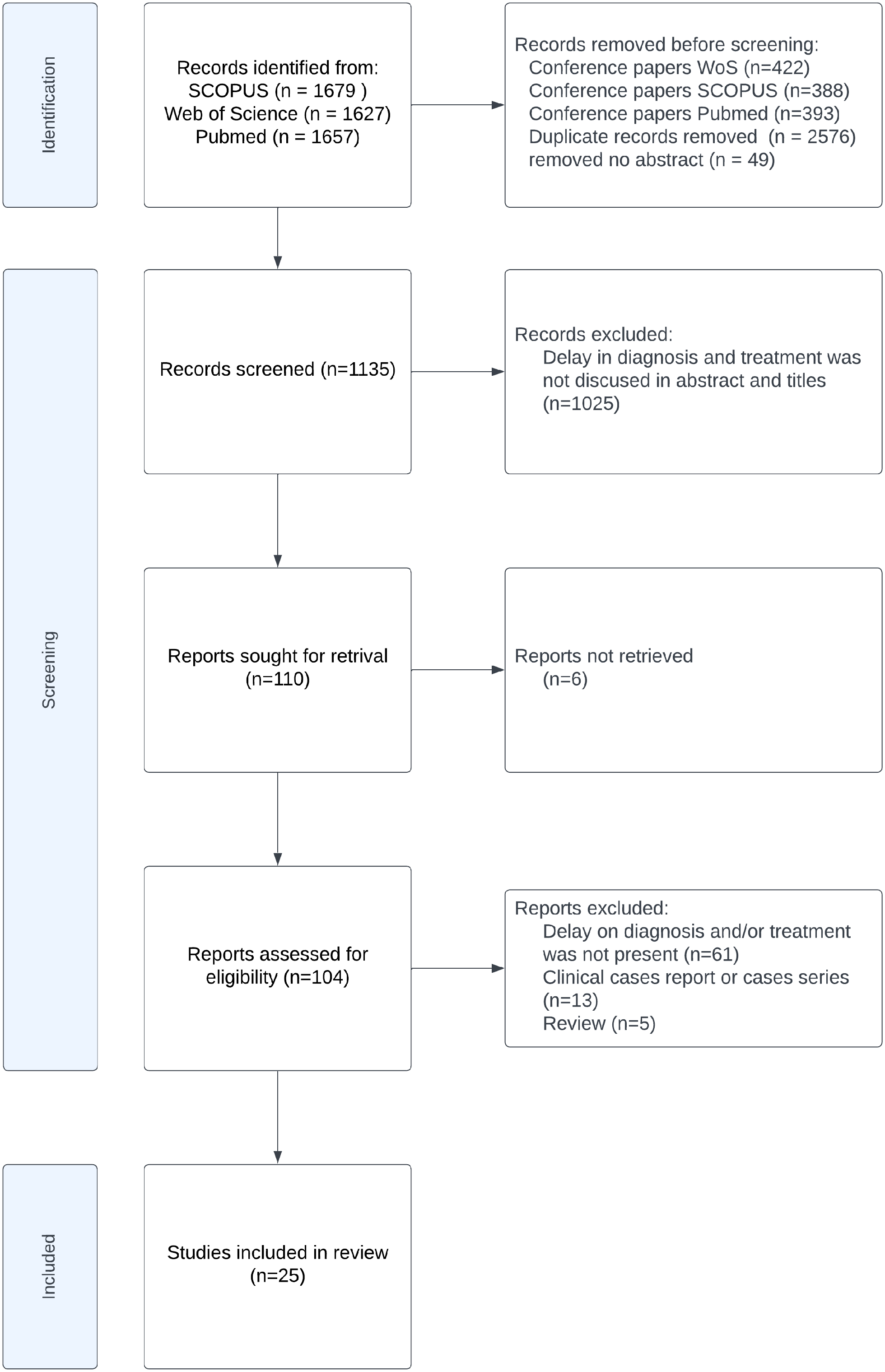
Results: Figure 1 illustrates the PRISMA search. A total of 25 studies were included, with an average quality of 6.36. The mean/median time to diagnosis is explicitly reported in 16 articles and can be estimated for 3 additional ones. Six articles presented a definition of SLE diagnostic delay, the most comprehensive being the time from symptom onset or sign verification to when diagnostic classification is fulfilled. Cut-off points for delay have historically been arbitrarily defined; only two studies clarified that theirs (>6 months) was established based on the literature, administrative data, and insurance databases.
The estimated mean delay in diagnosis was 25 months (19 studies), and the mean delay in treatment was 2.09 months (2 studies). The delay in diagnosis was 29 months in men and 43 months in women, reported in 5 articles. Early-onset SLE (diagnosis at <50 years of age) had a mean delay of 15.4 months, while delay in late-onset SLE was 16.7 months, reported in 3 studies. Black patients seek medical care sooner and experience less delay due to disease awareness and severe clinical manifestations; Caucasian and Mixed-race patients report longer delays. Patients with lupus nephritis are diagnosed earlier, likely due to more severe presentation. Contrastingly, long delays are related to neuropsychiatric symptoms and concomitant musculoskeletal/cardiorespiratory or mucocutaneous/haematological involvement. Delayed diagnosis and treatment are associated with severe damage accrual, disease activity, flares, hospitalizations, poor quality of life, greater use of resources, higher costs, and mortality.
The barriers identified for a timely diagnosis are: the number of physicians consulted before SLE diagnosis; misdiagnoses; lack of prompt access/referral to a specialist; lack of knowledge of the disease; rural setting; and expenses derived from medical care.
Conclusion: There is no consensus on how to define the delay in diagnosis and/or treatment in SLE patients, nor a unified method to estimate them. The variability in settings, patients, methods, and analyses complicates the attempt to unify the results and generalize them to diverse SLE patient populations worldwide. This Public Health problem needs to be urgently addressed, and context-specific barriers need to be identified and resolved.
REFERENCES: [1] Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Qureshi R, Mattis P, Lisy K, Mu P-F. Chapter 7: Systematic reviews of etiology and risk. In: Aromataris E, Munn Z (Editors). Joanna Briggs Institute Reviewer’s Manual. The Joanna Briggs Institute, 2017. Available from
PRISMA flow diagram of study selection
Acknowledgements: This protocol was registered with the international prospective register of systematic reviews (PROSPERO CRD42023456508).
Disclosure of Interests: None declared.