fetching data ... 
Background: In spite of significantly improved therapy during the last years, long-term morbidity and mortality has remained high in ANCA-associated vasculitis (AAV). The main causes of death within the first year after diagnosis are active vasculitis and infections, followed by cardiovascular disease, malignancies and infections during subsequent years [1-3]. Population-based database and cohort analyses suggest an increased risk for major adverse cardiovascular events (MACE) in AAV [4, 5].
Objectives: To assess risk of death and cardiovascular outcomes in AAV using a large global electronic health record database for biomedical and clinic research (TriNetX) [6].
Methods: In this retrospective cohort study, data samples from an electronic health records database of the US-based TriNetX network were analysed. Patients (aged≥18 years) with the diagnostic codes of granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA) (International Classification of Diseases [ICD]) and patients without vasculitis as matched control cohort (1:1) were included. Propensity score matching for demographic variables and cardiovascular and metabolic comorbidities was performed to optimize between-group comparability. Hazard ratios (HR) related to death and cardiovascular outcomes (MACE) were calculated by univariate Cox regression after analysis of the matched cohort by the Kaplan-Meier method. P values were determined by the Log-rank test.
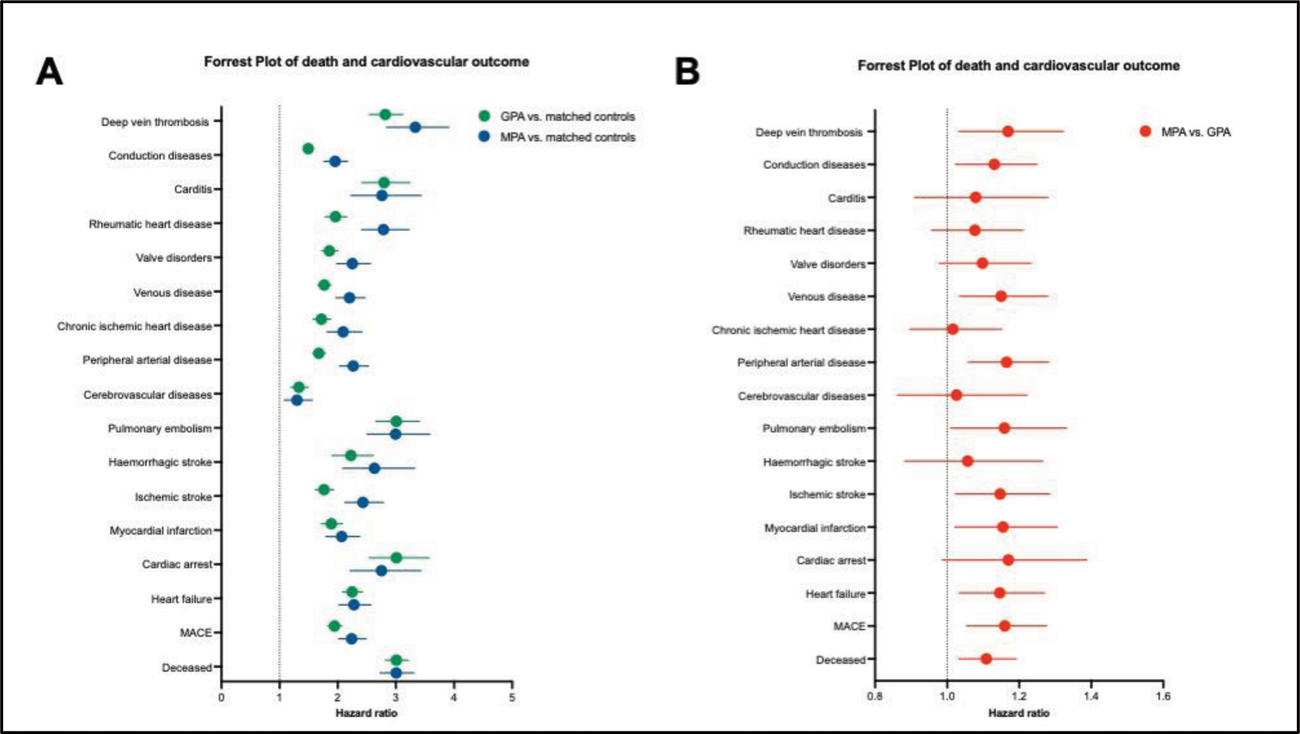
Results: We identified 21.190 patients with GPA and 5.907 with MPA. The unadjusted and adjusted relative risk (RR) of mortality was increased in GPA (RR 17.87%) and MPA (RR 25.85%) compared to matched controls (GPA: HR: 3.010 P < 0.0001, MPA: HR: 3.007, P < 0.0001; Figure 1A). The risks of all screened cardiovascular events were increased in GPA and MPA compared to matched controls (P < 0.0001; Figure 1A ) and did not differ when adjusted according to gender, disease duration (first 3 years after diagnosis), and age (patients < 46 years, patients > 64 years). Especially the risk for thromboembolic events was increased compared to matched controls (deep vein thrombosis: GPA HR: 2.819, MPA HR: 3.334; pulmonary embolism: GPA HR: 3.009, MPA HR: 2.997). Compared to GPA, MPA patients had a higher risk for MACE (MPA vs. GPA: 24.38% vs. 23.76%, HR: 1.160 P = 0.0023) and peripheral arterial disease (MPA vs. GPA: 21.38% vs. 21.17%, HR: 1.165 P = 0.0018; Figure 1B ).
Conclusion: In AAV, the risk of death and cardiovascular events were increased. Compared to GPA, MPA was associated with an increased risk for MACE and peripheral arterial disease.
REFERENCES: [1] Lamprecht P et al. Pathogenetic and clinical aspect of anti-neutrophil cytoplasmic autoantibody-associated vasculitides . Front Immunol. 2018 Apr 9;9:680.
[2] Sanchez-Alamo B et al. Long-term outcomes and prognostic factors for survival of patients with ANCA-associated vasculitis. Nephrol Dial Transplant. 2023;38_1655-1665.
[3] Flossmann O et al. Long-term patient survival in ANCA-associated vasculitis. Ann Rheum Dis. 2011;70:488-494.
[4] Aviña-Zubieta JA et al. Risk of Myocardial infarction and stroke in patients with granulomatosis with polyangiitis (Wegener’s): A population-based study. Arthritis Rheumatol. 2016 Nov;68(11):2752-2759.
[5] Massicotte-Azarnioch D et al. Association of anti-neutrophil cytoplasmic antibody-associated vasculitis and cardiovascular events: a population-based cohort study. Clin Kidney J. 2021 Nov 24;15(4):681-692.
[6] Palchuk et al. A gobal federated real-world data and analytics platform for research. JAMIA Open 2023;6(2).
Forest plot based on hazard ratios of death and all cardiovascular outcomes. A: Elevated risk of death and cardiovascular events in GPA (green) and MPA (blue) compared to matched controls; B: Comparison of risks for MACE and peripheral arterial disease between MPA and GPA ( P = 0.0023).
Acknowledgements: NIL.
Disclosure of Interests: None declared.