fetching data ... 
Background: Takayasu’s arteritis (TA) is often complicated with reno-vascular hypertension. Renal revascularization can be used to treat resistant hypertension in TA. Renal revascularization is done using percutaneous transluminal angioplasty, renal artery bypass with an in-situ hepatic, splenic artery or a saphenous vein graft with an aortic inflow [1]. We report a case of resistant hypertension due to bilateral renal artery stenosis in TA, treated with autologous renal transplant.
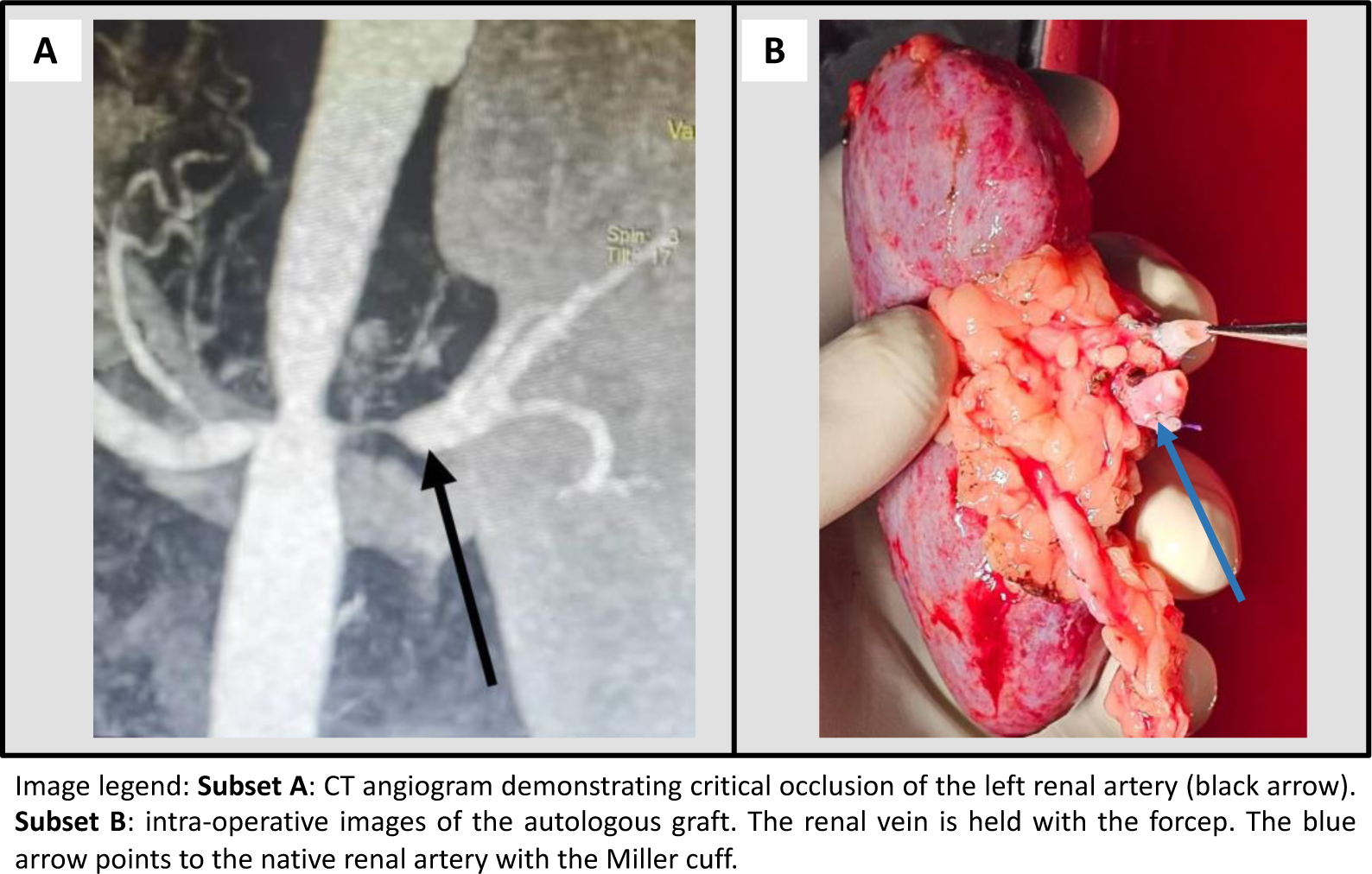
Case presentation: A 29-year-old Sri Lankan female with TA and resistant hypertension was found to have 90% and 25% luminal obstruction in the left and right renal arteries respectively (Figure 1: subset A). Despite treatment with prazosin 5.5mg thrice daily, cilnidipine 10 mg daily, methyldopa 500mg thrice daily, metoprolol 50mg twice daily, and spironolactone 50mg once daily, her blood pressure was persistently higher than 180/90 mmHg in the right arm. She was on prednisolone 60mg and azathioprine 100mg daily. Her renal functions and the DTPA scan were normal. She did not tolerate renin-aldosterone inhibitors. Stenting of the left renal artery was failed. She underwent an autologous left renal transplant to the right internal iliac artery using a Miller cuff (Figure 1: subset B). She was treated with IV tocilizumab to reduce vascular friability, preoperatively. After surgery, her blood pressure was controlled with metoprolol 25mg twice daily and cilnidipine 10mg daily alone.
Learning points for clinical practice: Renal auto-transplantation can be used to treat resistant reno-vascular hypertension in Takayasu’s arteritis if not amenable for endo-vascular therapies.
REFERENCES: [1] Ogino H, Matsuda H, Minatoya K, Sasaki H, Tanaka H, Matsumura Y, Ishibashi-Ueda H, Kobayashi J, Yagihara T, Kitamura S. Overview of late outcome of medical and surgical treatment for Takayasu arteritis. Circulation. 2008 Dec 16;118(25):2738-47. doi:10.1161/CIRCULATIONAHA.107.759589. PMID:19106398.
Acknowledgements: NIL.
Disclosure of Interests: None declared.