fetching data ... 
Background: Sjögren disease (SjD) is the autoimmune disease with the highest risk of lymphoma. The most common histology is marginal zone (MZ) lymphoma particularly the mucosa-associated lymphoid tissue (MALT) lymphoma. There is a continuum between autoimmunity and lymphoma, and disease activity is a major risk factor for lymphoma development. Managing lymphoma complicating SjD remains non-consensual with different options: wait and watch, local or systemic therapy.
Objectives: To describe characteristics of non-Hodgkin lymphoma in Sjögren disease (SjD), therapeutic strategies, and the impact of these strategies on the prognosis of lymphoma and SjD.
Methods: This multicentric retrospective study included all lymphoma patients of the ASSESS prospective cohort, enriched with patients recruited in 15 French Rheumatology and Internal Medicine departments. We collected biological and clinical manifestations of SjD, lymphoma characteristics, and treatment strategy. Exploratory analysis identified factors associated with lymphoma relapse, SjD relapse and overall survival (OS). Propensity scores were created using key clinical variables to compare patients depending on treatment strategy. Three outcomes were analyzed: lymphoma progression-free survival (Lymphoma-PFS), Sjögren Disease progression-free survival (SjD-PFS), and OS.
Results: One hundred and six patients were included. The most frequent histological subtype was MZ lymphoma (82 patients) including 68 MALT, followed by 14 diffuse large B cell lymphoma.
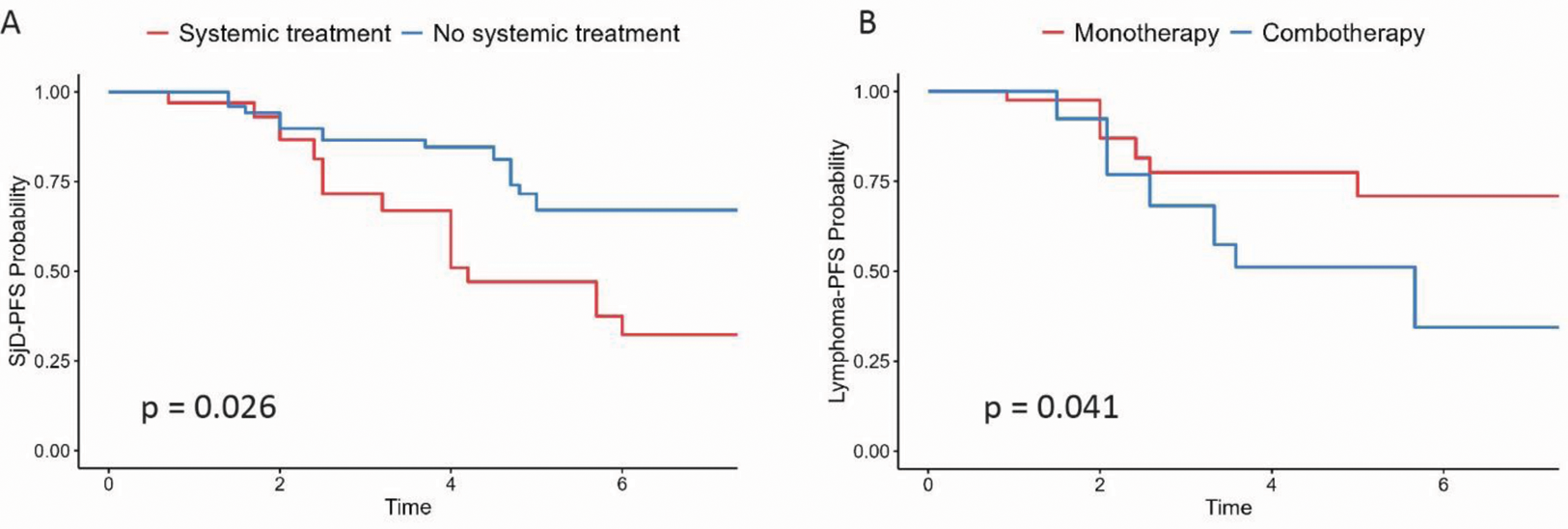
Among the 82 patients with MZ lymphoma, after multivariate adjustment on age, localization, Bendamustine use, Ann arbor stage and calendar year at lymphoma diagnosis, older age and pulmonary involvement were negatively associated with overall survival (HR 1.15 CI 95% [1.05-1.26] and HR 6.40 CI 95% [1.10-37.1]). We did not find individual factors associated with lymphoma or SjD-PFS. Fifty (61%) MZ patients received systemic treatment with chemotherapy and/or rituximab. These patients had more frequently pulmonary lymphoma locations (24% vs 3.1%, p = 0.012) and tended to have higher SjD disease activity at lymphoma diagnosis. After a median follow-up of 7 years, 26 patients (32%) experienced lymphoma relapse, 9 (11%) died, and 27 (33%) experienced SjD relapse. After propensity score adjustment, patients treated with first line systemic treatments for lymphoma, displayed a longer SjD progression-free survival (PFS) (HR=0.43 [95% CI 0.21-0.90], p = 0.026) than patients without systemic treatment (including watch and wait strategy or local treatment alone). There was no difference in lymphoma relapse nor overall survival. Patients treated with first-line combo-therapy (anti-CD20 and chemotherapy) had a longer lymphoma-PFS than patients with first-line monotherapy (anti-CD20 or chemotherapy): HR 0.36 [95% CI 0.14-0.96], p = 0.041. There was no difference in SjD-PFS or overall survival between the two groups. Of note, none of the patients with anti-CD20 maintenance therapy relapsed (0% vs 36%, log-rank p = 0.04)
Conclusion: In patients with SjD and MZ lymphoma, older age and pulmonary involvement were negatively associated with OS. Systemic first-line treatment of lymphoma reduced the risk of SjD relapse suggesting that in case of indecisiveness between treatment and watch and wait attitude, activity of SjD beyond lymphoma is a strong argument in favor of a systemic treatment. A combination of B-cell targeted therapy and chemotherapy may be considered for decreasing the risk of lymphoma relapse.
A) Probability of Sjögren progression free survival according to systemic treatment vs no systemic treatment at lymphoma diagnosis, after propensity score adjustment. B) Probability of Lymphoma-PFS according to combotherapy vs monotherapy, after propensity score adjustment.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Maxime Beydon: None declared, Juliette Rocca: None declared, Véronique Le Guern: None declared, Eric Hachulla: None declared, Marion Couderc: None declared, Sandrine Jousse-Joulin: None declared, Valerie Devauchelle-Pensec: None declared, Jacques-Eric Gottenberg Abbvie, Astra Zeneca, Sanofi, Lilly, Galapagos, Gilead, Roche Chugai, Pfizer, Bristol Myer Squib, MSD, Pfizer, Abbvie, Lilly, Olivier Vittecoq: None declared, Christian Lavigne: None declared, Jean Schmidt: None declared, Claire Larroche: None declared, Xavier Mariette Astra Zeneca, Bristol Myer Squib, Galapagos, GSK, Novartis and Pfizer, Raphaèle Seror GSK, Bristol Myer Squib, Boerhinger and Janssen, Gaetane Nocturne: None declared.