fetching data ... 
Background: Disease activity in systemic lupus erythematosus (SLE) increases the risk of accrued damage and cardiovascular risk. Endothelial biomarkers, such as VEGF, CD54, CD62P, and fractalkine (CX3CL1), play crucial roles in endothelial dysfunction, vascular inflammation, and immune cell recruitment. Additionally, these molecules are involved in the maturation and chemotaxis of endothelial progenitor cells (EPCs), positioning them as potential mediators in SLE pathogenesis. Therefore, assessing these biomarkers could provide insights into disease activity and accrued damage.
Objectives: Our aim was to evaluate the levels of these biomarkers in SLE patients and analyze their relationships with disease activity and accrued damage.
Methods: A cross-sectional study was conducted in which plasma levels of VEGF, CD54, CD62P, and fractalkine were compared between SLE patients and healthy controls (HC). Clinical and analytical variables were measured, and biomarkers were correlated with disease activity and the Systemic Damage Index (SDI). Biomarkers were measured by flow cytometry using a cytometric bead array (CBA-BD).
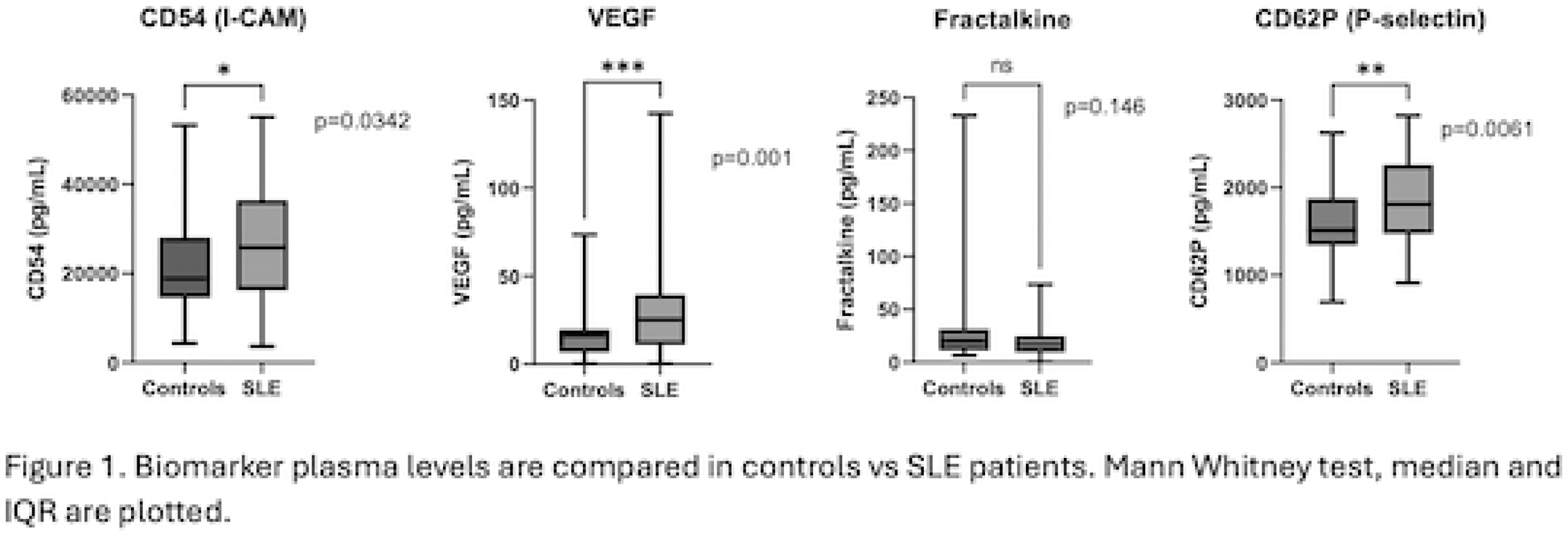
Results: A total of 50 patients and 34 HC were included. The baseline characteristics are summarized in Table 1. Higher levels of VEGF, CD54, and CD62P were observed, while no differences in fractalkine levels were noted (Figure 1). No significant differences were found between cytokine levels and cardiovascular risk factors (CVRF), nor in the domains of involvement, presence of active nephritis, SLEDAI, any SDI, complement levels, DNA, or proteinuria. Lower levels were observed in patients receiving immunosuppressive therapy (1736.8 pg/mL, IQR 1482.4 – 2041.6 vs. 2219.4 pg/mL, IQR 1901.4–2623.8; p=0.03).
Conclusion: Our findings are consistent with previous reports regarding cytokine levels in SLE compared to healthy controls, highlighting the role of chronic inflammation and endothelial damage. However, no associations were found between these biomarkers and disease activity, accrued damage, or cardiovascular risk factors. This may, in part, be explained by the characteristics of the cohort, which was predominantly younger and had a low incidence of CVRF and active nephritis. Our findings underscore the relationship between immunosuppressive therapy and CD62P levels, which may have implications for the prevention of vascular damage. However, these findings need to be confirmed in larger, prospective studies.
REFERENCES: NIL.
Demographic and Clinical Features
| SLE patients (n=50) | Controls (n=34) | p value | |
|---|---|---|---|
| Age (years) (median (IQR)) | 33 (27 – 38) | 29 (27 – 36) | 0.496 |
| Gender (female) | 39 (78%) | 21 (61.8%) | 0.776 |
| CV risks factors | 16 (32%) | 8 (23.5%) | 0.586 |
| Hypertension (n, %) | 8 (16%) | 1 (2.9%) | 0.264 |
| Diabetes (n, %) | 0 (0%) | 0 (0%) | NA |
| Dyslipidemia (n, %) | 2 (4%) | 2 (5.9%) | 0.574 |
| Smoking (n, %) | 5 (10%) | 5 (14.7%) | 0.141 |
| Obesity (n, %) | 1 (2%) | 0 (0%) | 1.0 |
| Clinical and serological characteristics | |||
| Time disease evolution (years) (median (IQR) | 6 (3 – 12) | NA | |
| C3 mg/dL (median (IQR)) | 84 (65 – 103) | NA | |
| C4 mg/dL (median (IQR)) | 12 (7 – 22) | NA | |
| Anti-double stranded DNA (n, %) | 21 (42%) | NA | |
| SLEDAI (median (IQR)) | 4 (2 – 8) | NA | |
| SLEDAI ≥ 3 (n, %) | 29 (58%) | NA | |
| SDI ≥1 (n, %) | 10 (20%) | NA | |
| Kidney involvement | 21 (42%) | NA | |
| Active lupus neprhitis | 11 (22%) | NA | |
IQR: interquartile range. CV: cardiovascular, Obesity was defined as BMI >30, SLEDAI: SLE disease activity index; SDI: Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index; NA: not applicable.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (