fetching data ... 
Background: Pre-eclampsia (PE) is one of the leading causes of maternal and fetal morbidity and mortality. With a prevalence of 2-5%, its onset has been linked to advanced maternal age, specific ethnic groups, and certain cardiovascular or obstetric factors. Additionally, the pro-inflammatory and pro-thrombotic environment characteristic of systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS) contributes to a heightened risk for developing PE. Nevertheless, SLE is a highlyheterogeneous disease, and the propensity for developing PE can vary significantly depending on specific disease features, such as a prior history of lupus nephritis (LN).
Objectives: To evaluate the impact of APS and SLE, with a particular focus on LN, on the risk of developing PE and PE with severity criteria.
Methods: A nationwide descriptive analysis of pregnancy-related hospitalizations was conducted using the Spanish National Hospital Discharge Database (SNHDD). This database includes demographic, epidemiological, and clinical data coded using the ICD-10. Pregnancy-related admissions were identified using ICD codes for pregnancy-related disorders (O00-O99). Additional conditions and obstetric features associated with the development and severity of PE were also retrieved from the patients’ diagnostic records, including SLE, LN and APS. Binary logistic regression analyses were performed to evaluate factors independently associated with the development of PE and PE with severity criteria (PESC). The variables considered included age over 35, Black-African, Hispanic, and Polynesian ethnicity, previous adverse obstetric outcomes (PRAOO), assisted reproductive techniques (ART), twin pregnancy, baseline high blood pressure (HBP), diabetes mellitus (DM), obesity, SLE, LN, and APS. PESC was defined as early-onset PE, severe PE, eclampsia, or HELLP syndrome. Statistical significance was set at p<0.05.
Results: A total of 1,979,249 admissions for pregnant patients between 2016-2022 were retrieved from the database. Among these, 1,787 patients had SLE (0.1%), with prior LN reported in 13.2% of them (Table 1). Compared to non-SLE patients, pregnant women with SLE were older (mean age 33.9 vs 32.1), and exhibited higher rates of baseline HBP (5.8% vs 1.1%), APS (9.3% vs 0.1%), PRAOO (4.1% vs 2.2%), ART (2.6% vs 1.5%), and twin pregnancies (4% vs 2.4%) (p<0.001 for all). Conversely, they showed a lower rate of DM (4.3% vs 6.3%; p<0.001). A total of 42,050 (2.1%) of pregnancies developed PE, with severity criteria identified in 12,421 (29.5%). Pregnant women with SLE suffered higher rates of PE (5.5% vs 2.1%) and PESC (2.1% vs 0.6%), including early onset PE (0.5% vs 0.1%), severe PE (1.3% vs 0.5%) and HELLP syndrome (2.1% vs 0.6%) (p<0.001 for all). After adjustment, an increased risk of PE and PESC was identified in patients with SLE (OR=1.78, 95% CI 1.39-2.28; OR=2.17, 95% CI 1.47-3.22, respectively), LN (OR=1.94, 95% CI 1.18-3.19; OR=2.45, 95% CI 1.18-5.09, respectively) and APS (OR=1.53, 95% CI 1.28-1.84; OR=1.91, 95% CI 1.44-2.54, respectively) (Figure 1). In SLE patients, only HBP (OR=4.27, 95% CI 2.45-7.44), LN (OR=2.06, 95% CI 1.26- 3.37) and APS (OR=1.85, 95% CI 1.03-3.32) were associated with PE. Furthermore, LN (OR=2.88, 95% CI 1.41-5.91) was the sole risk factor for PESC in the multivariate analysis.
Conclusion: Whilst patients with SLE exhibit a higher risk of PE and PESC compared to the general population, this risk is further amplified in those with a history of LN or APS. Notably, among individuals with SLE, only HBP, LN, and APS contribute to an increased risk of developing PE, with LN independently associated with an increased risk of PESC. Despite the intrinsic methodological limitations of this study, our findings underscore the importance of rigorous preconception management, comprehensive risk stratification for PE, and meticulous monitoring during pregnancy in patients with a history of LN or APS.
Populations characteristics and outcomes
| Total | SLE | Non-SLE | p-value | |
|---|---|---|---|---|
| Age (years, mean, SD) | 32.1 (5.9) | 33.9 (5.1) | 32.1 (5.9) | <0.001 |
| HBP (n, %) | 21,383 (1) | 104 (5.8) | 21,279 (1.1) | 0.001 |
| DM (n, %) | 124,128 (6.3) | 77 (4.3) | 124,051 (6.3) | <0.001 |
| Obesity (n, %) | 77,109 (3.9) | 68 (3.8) | 77,041 (3.9) | 0.895 |
| APS (n, %) | 2,957 (0.1) | 166 (9.3) | 2,791 (0.1) | <0.001 |
| PRAOO (n, %) | 42,935 (2.2) | 73 (4.1) | 42,862 (2.2) | <0.001 |
| ART (n, %) | 29,110 (1.5) | 46 (2.6) | 29,064 (1.5) | <0.001 |
| Twin pregnancy (n, %) | 47,263 (2.4) | 71 (4) | 47,192 (2.4) | <0.001 |
| Pre-eclampsia | 42,050 (2.1) | 99 (5.5) | 41,951 (2.1) | <0.001 |
| With severity criteria | 12,421 () | 37 () | 12,384 () | <0.001 |
| ICU admission | 11,362 (0.6) | 17 (1) | 11,345 (0.6) | 0.042 |
| Death | 126 (<0.1) | 0 | 126 (<0.1) | 1 |
SLE: Systemic lupus erythematosus; HBP: High blood pressure; DM: Diabetes mellitus, APS: Antiphospholipid syndrome; PRAOO: Previous adverse obstetric outcome; ART: Assisted reproduction techniques; PE: Pre-eclampsia.
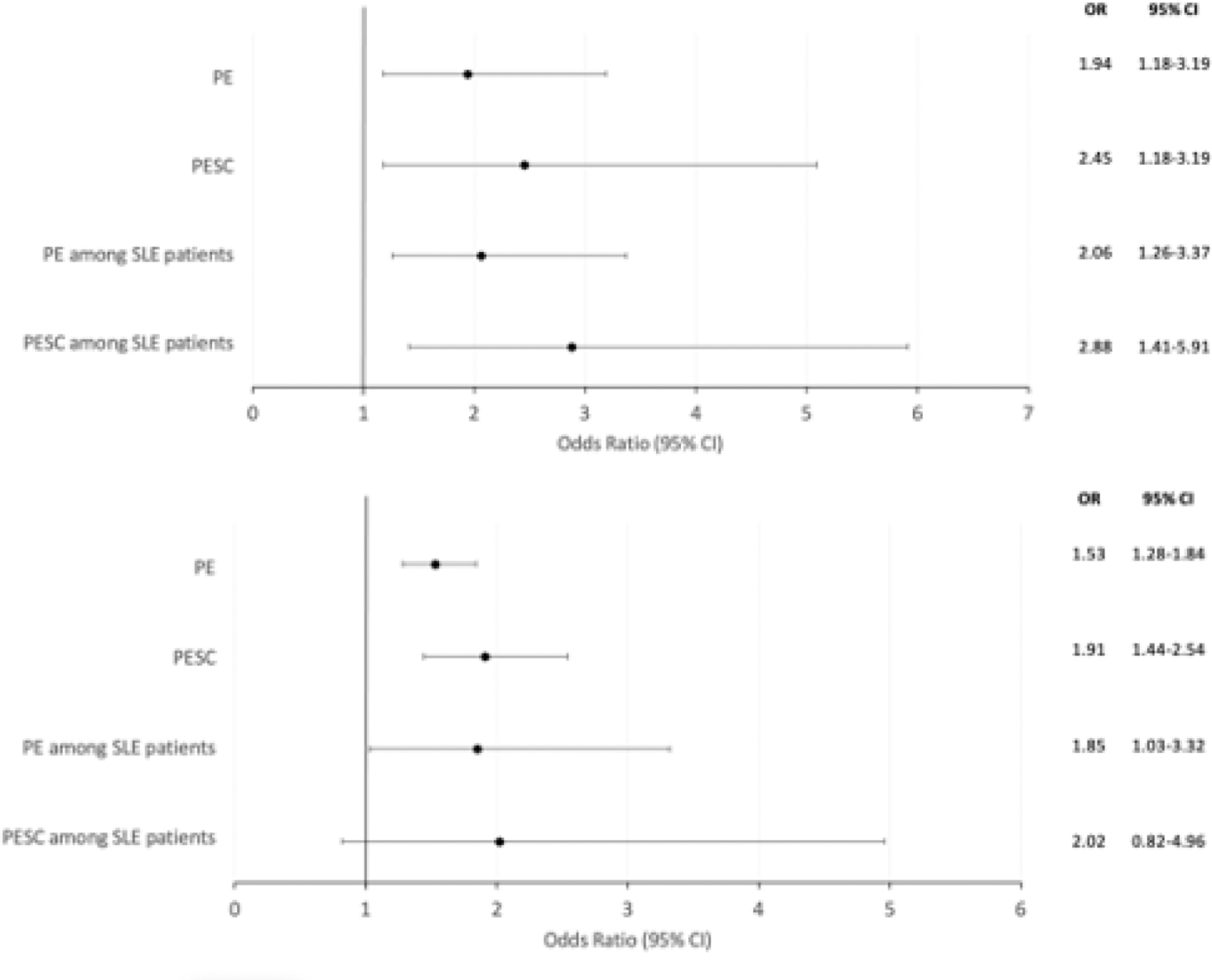
Impact of lupus nephritis (A) and antiphospholipid syndrome (B) on pre-eclampsia risk and severity.
The figure shows the impact of lupus nephritis (A) and antiphospholid syndrome (B) on pre-eclampsia (PE) and pre-eclampsia with severity criteria (PESC) after adjustment. The variables considered were age over 35, Black-African, Hispanic, and Polynesian ethnicity, previous adverse obstetric outcomes, assisted reproductive technique, twin pregnancy, baseline high blood pressure, diabetes mellitus and obesity, as well as systemic lupus erythematosus for the general population.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (