fetching data ... 
Background: Systemic lupus erythematosus (SLE) is an autoimmune disease with diversity of autoantibodies and clinical manifestation. The identification of patient clusters by autoantibody profile can predict prognosis and mortality.
Objectives: The aim of this study is to define and describe serological clusters and their clinical and epidemiological characteristics, as well as their association with comorbidities, disease activity, severity and damage.
Methods: Descriptive, observational and multicenter study that includes patients with SLE from the Spanish national registry RELESSER. 1740 patients were included in the cross-sectional study and 718 in the prospective study (with annual follow-up during 5 years). The autoantibodies selected for cluster analysis were anti-deoxyribonucleic acid (anti-DNA), anti-Smith (anti-Sm), anti-ribonuclear proteins (anti-RNP), anti-Ro, anti-La and antiphospholipid antibodies. Cluster analysis was carried out using Gower distance. To compare the distributions of categorical variables, Chi-square tests were used or Fisher’s exact test in cases of low expected frequencies. For continuous variables, non-parametric tests such as Kruskal-Wallis or ANOVA were applied, depending on the data distribution and homogeneity of variances.
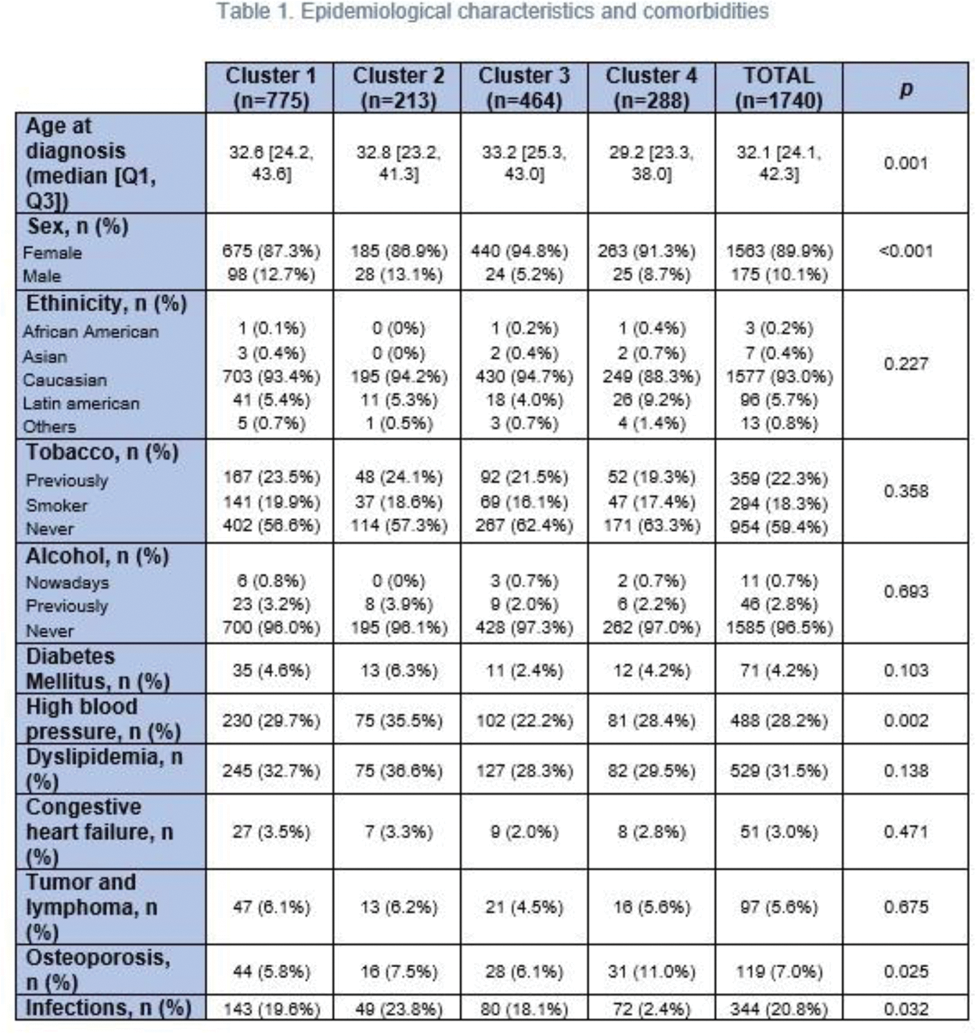
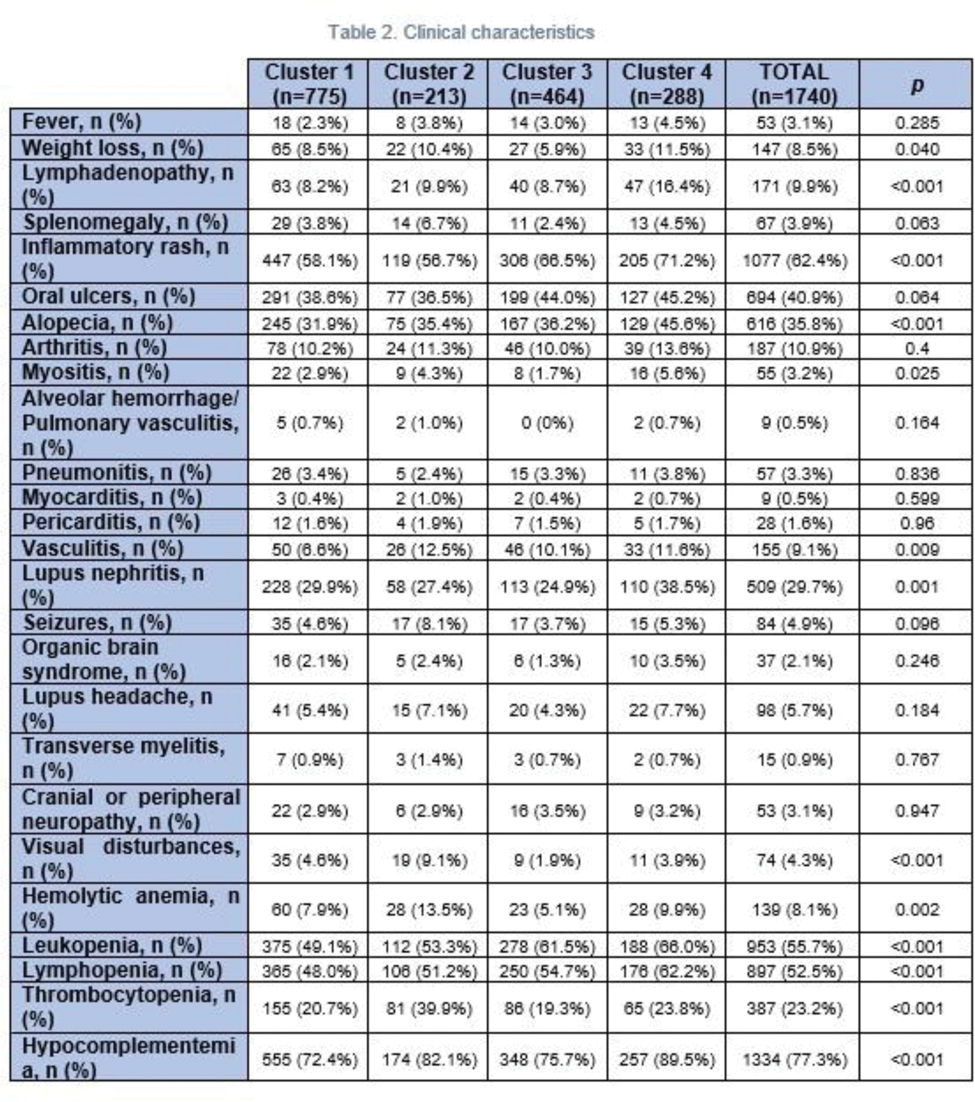
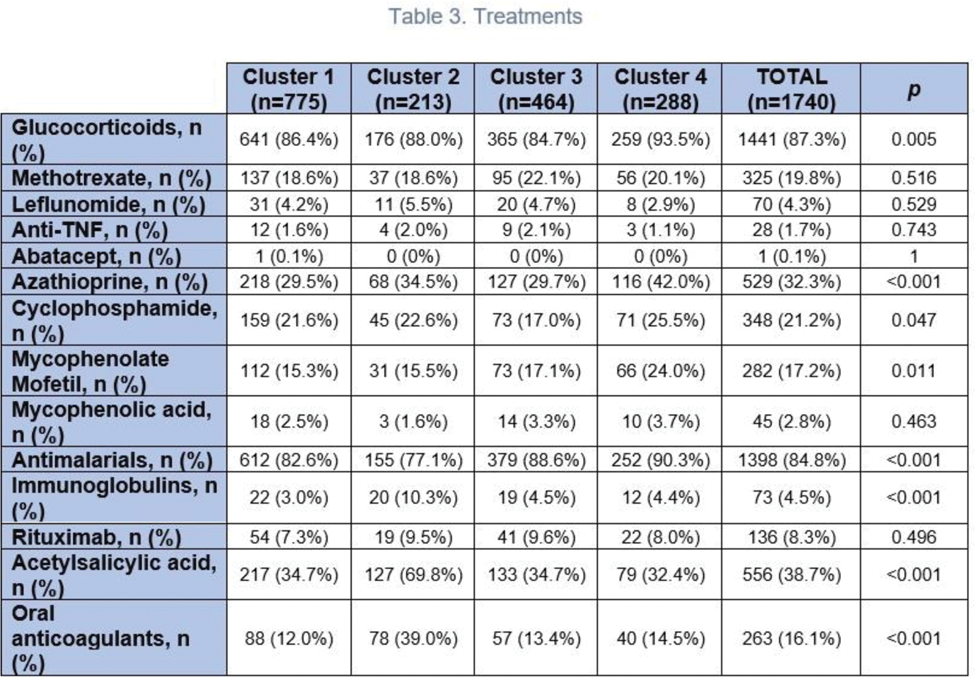
Results: Four serological clusters were defined. Cluster 1 (absence of anti-extractable nuclear antigen antibodies; 44.54% of the patients) was characterized by lower frequency of vasculitis (6.6%), leukopenia (49.1%) and lymphopenia (48.0%). Cluster 2 (antiphospholipid antibodies; 12.24%) was represented by higher frequency of high blood pressure (35.5%) as well as hemolytic anemia (13.5%), thrombocytopenia (39.9%), vasculitis (12.5%), visual disturbances (9.1%) and higher use of immunoglobulins (10.3%) and oral anticoagulants (39.0%). Cluster 3 (anti-Ro and anti-La; 26.67%) had the lowest frequency of lupus nephritis (24.9%). Patients from cluster 4 (anti-Sm and anti-RNP; 16.55%) were younger at disease onset (median age of 29.2 years) and had the highest frequency of lupus nephritis (38.5%), leukopenia (66.0%), lymphopenia (62.2%), hypocomplementemia (89.5%), myositis (5.6%) and cutaneous manifestations. Besides, they had a higher frequency of osteoporosis (11.0%) and severe infections (26.4%) and a higher use of glucocorticoids (93.5%), azathioprine (42.0%), cyclophosphamide (25.5%) and mycophenolate mofetil (24.0%). Regarding disease activity assesed by SLEDAI (Systemic Lupus Erythematosus Disease Activity Index), at visit 1 of the longitudinal study, patients in cluster 4 had the highest scores: 2.5 ± 3.37 (1.70 ± 3.09 in cluster 1 (p=0.18), 2.18 ± 4.26 in cluster 2 (p=0.4), 1.86 ± 2.50 in cluster 3 (p=0.011)). After 5 years of follow-up, no differences were observed between clusters. Concerning damage assessed by SLICC/ACR DI (Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index), patients in cluster 2 exhibited the highest scores at visit 1: 1.93 ± 2.30 (1.42 ± 1.81 in cluster 1 (p=0.018), 1.13 ± 1.72 in cluster 3 (p<0.001), 1.67 ± 1.92 in cluster 4 (p=0.4)). After 5 years of follow-up, a significant increase was observed across all clusters (p<0.001), with differences between clusters persisting at the end of follow-up (p=0.049). Regarding severity measured by Katz, patients in cluster 4 had the highest scores at visit 1: 5.24 ± 2.09 (4.45 ± 2.13 in cluster 1 (p<0.001), 4.57 ± 2.20 in cluster 2 (p=0.019), 4.35 ± 1.69 in cluster 3 (p<0.001)). The differences persisted after follow-up (p=0.005). As for mortality, 21 deaths were recorded: 5 in cluster 1 (1.74%), 6 in cluster 2 (5.50%), 6 in cluster 3 (2.97%) and 4 in cluster 4 (3.36%), with no significant differences between clusters (p=0.427).
Conclusion: In our cohort, the serological profile constitutes a crucial factor for the clinical stratification of patients and predicting their prognosis. Nevertheless, further studies are required to facilitate a more precise identification and comprehensive understanding of these patients.
REFERENCES: [1] To CH, Petri M. Is antibody clustering predictive of clinical subsets and damage in systemic lupus erythematosus? Arthritis Rheum. 2005 Jun;52(12):4003–10.
[2] Artim-Esen B, Çene E, Şahinkaya Y, Ertan S, Pehlivan Ö, Kamali S, et al. Cluster Analysis of Autoantibodies in 852 Patients with Systemic Lupus Erythematosus from a Single Center. J Rheumatol. 2014 Jun;41(7):1304–10.
[3] Choi MY, Chen I, Clarke AE, Fritzler MJ, Buhler KA, Urowitz M, et al. Machine learning identifies clusters of longitudinal autoantibody profiles predictive of systemic lupus erythematosus disease outcomes. Ann Rheum Dis. 2023 Jul;82(7):927–36.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (