fetching data ... 
Background: Systemic lupus erythematosus (SLE) is an autoimmune disorder marked by chronic inflammation and immune dysregulation, significantly increasing the cardiovascular (CV) risk. Sleep duration is a key factor in cardiovascular health, with both insufficient and excessive sleep linked to adverse outcomes. Short sleep has been associated with increased obesity, hypertension, and other CV risks. Despite growing evidence highlighting the role of sleep in cardiac function, its specific impact on echocardiographic parameters, such as left ventricular mass index (LVMI), relative wall thickness (RWT), and measures of systolic and diastolic function, remains poorly understood.
Objectives: Determine the association between sleep time and alterations in the left ventricle’s geometry, diastolic function, and systolic function in patients with SLE.
Methods: A cross-sectional and comparative study was conducted on women with SLE, aged 18 years or older, who met the 2019 ACR/EULAR criteria. Patients with prior CV disease, pregnancy, and overlap syndrome were excluded. Patients were categorized into two groups based on their sleep duration, as determined through history: those with less than 7 hours (<7 hours) and those with 7 or more hours (≥7 hours) of nighttime sleep. Echocardiographic measurements were made using B-mode, M-mode, Spectral Doppler, Color Doppler, and Tissue Doppler Imaging. Cardiac geometry, diastolic function, and systolic function were classified according to the 2016 ASE/EACVI criteria. The normality was assessed with the Kolmogorov-Smirnov test. Comparisons were performed using the Student’s T-test, Chi-square test, and Mann-Whitney U test, accordingly. CV risk factors that were related to ventricular geometry and systolic function were included in a multivariable logistic regression. A p-value of ≤0.05 was considered statistically significant.
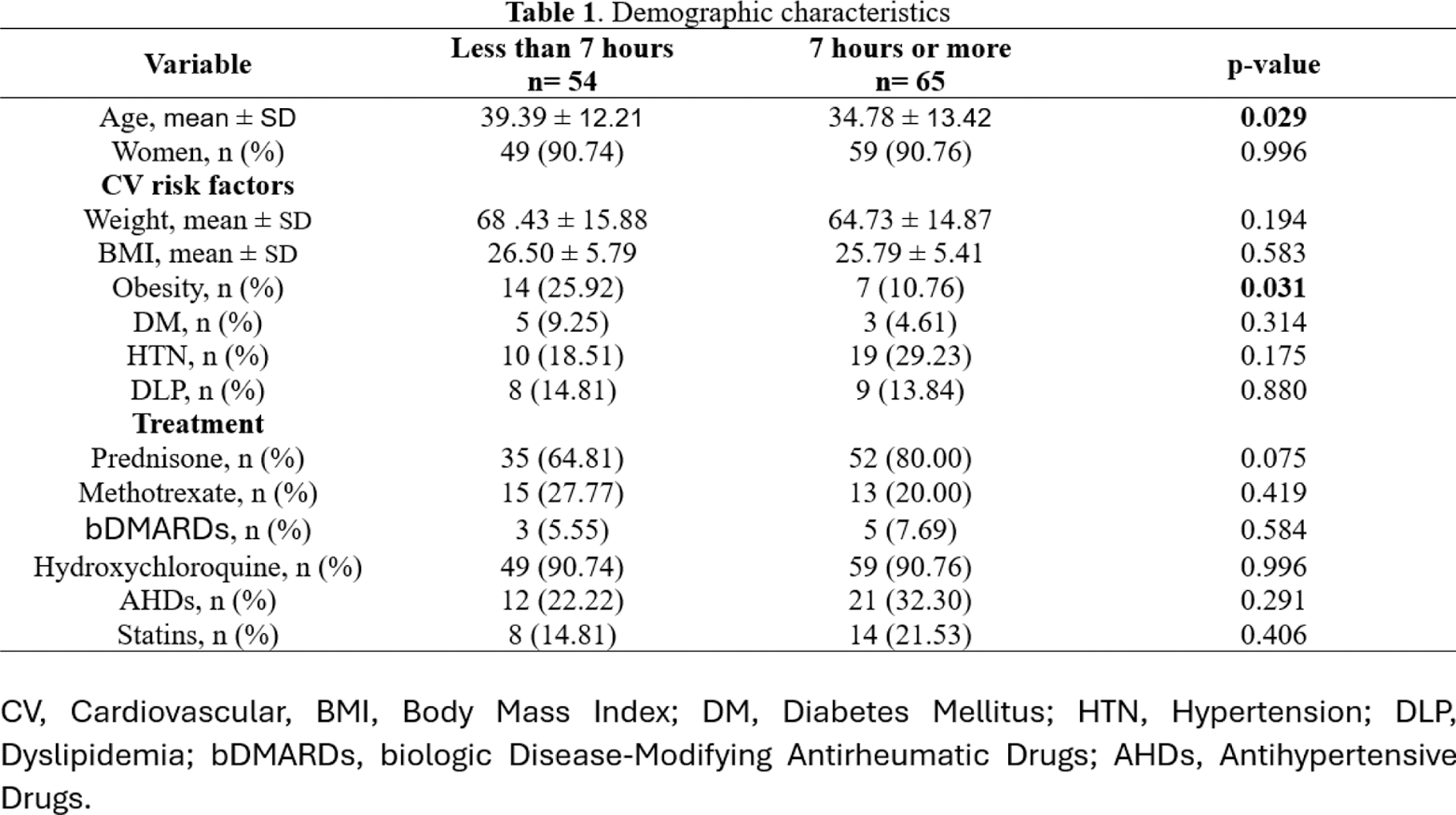
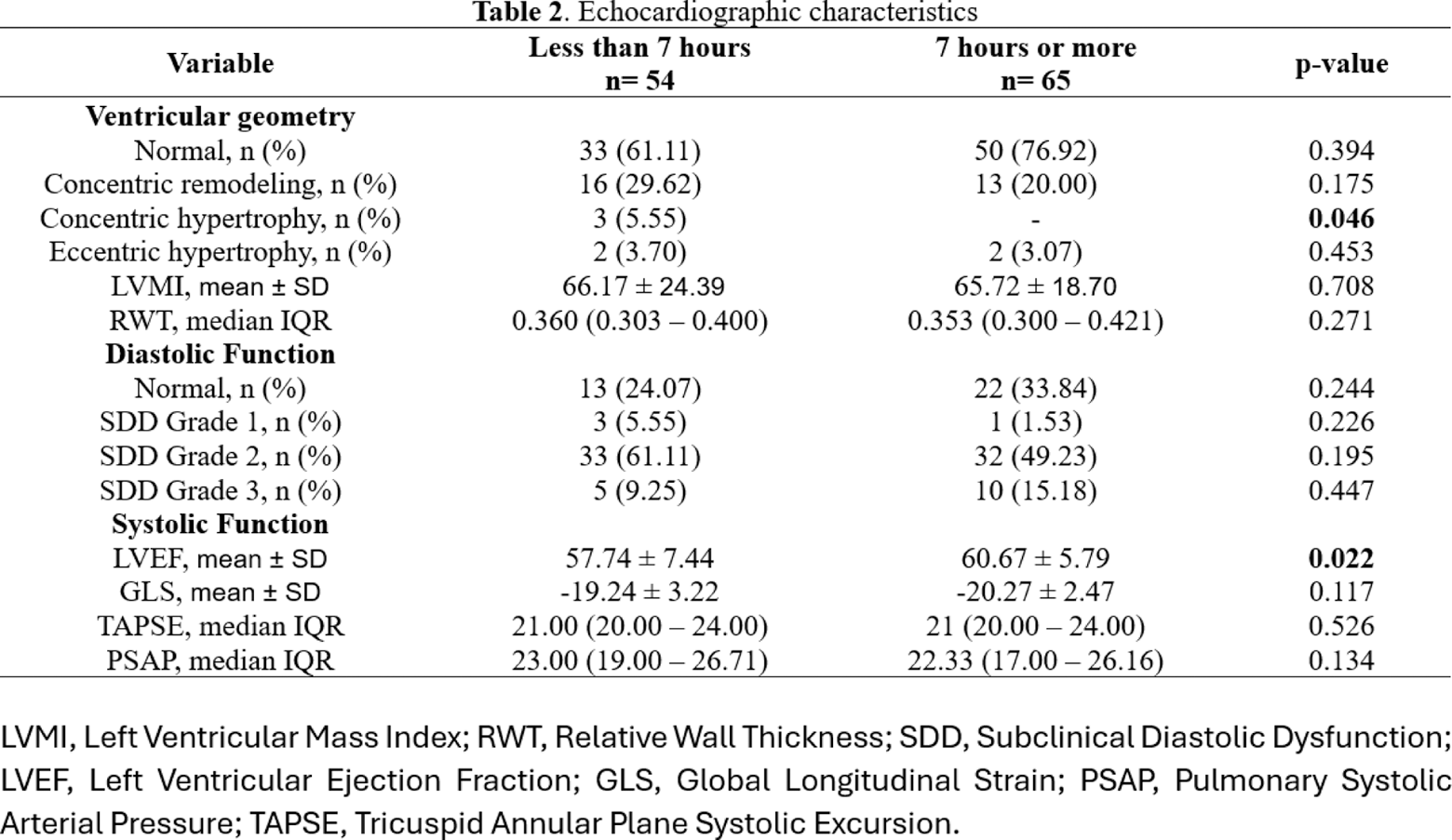
Results: A total of 119 patients were recruited. Those with shorter sleep time had a significantly higher mean age (39.39 ± 12.21 vs. 34.78 ± 13.42 years, p=0.029) and a greater prevalence of obesity (25.92% vs. 10.76%, p=0.031). Cardiovascular (CV) risk factors such as diabetes mellitus and dyslipidemia were similar between the groups. However, hypertension was more prevalent in the ≥7-hour group (29.23% vs. 18.51%), though this difference did not reach statistical significance (p=0.175). Regarding echocardiographic parameters, both groups had comparable ventricular geometry and left ventricular mass index (LVMI). Subclinical diastolic dysfunction (SDD) grade 2 was the most common in both groups, with similar prevalences (61.11% in the <7-hour group vs. 49.23% in the ≥7-hour group, p=0.195). However, concentric hypertrophy was observed exclusively in the <7-hour group (p=0.046). Concerning the result of the SDD Grade 3 values, as it showed an opposite trend to what we expected, we decided to perform a multivariable logistic regression which demonstrated that higher hypertension rates were associated with this variable (OR 1.051, 95% CI: 0.399-0.815, p = 0.047). Systolic function was slightly better in the ≥7-hour group, with a significantly higher left ventricular ejection fraction (LVEF) (60.67 ± 5.79 vs. 57.74 ± 7.44, p=0.022), while global longitudinal strain (GLS) and tricuspid annular plane systolic excursion (TAPSE) did not differ between groups.
Conclusion: This study displays notable differences in demographic, CV risk, and echocardiographic profiles based on sleep duration. Overall, patients with shorter sleep duration demonstrated a higher prevalence of obesity and concentric hypertrophy, with lower systolic function. Therefore, the standardized use of echocardiography in the comprehensive CV assessment of these patients would enable better risk stratification and an enhanced ability to implement personalized preventive measures, helping to avoid long-term CV complications.
REFERENCES: [1] Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, Van Den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34(11):1487–92.
[2] Mirbagher L, Gholamrezaei A, Hosseini N, Sayed Bonakdar Z. Sleep quality in women with systemic lupus erythematosus: contributing factors and effects on health‐related quality of life. Int J Rheum Dis. 2016;19(3):305–11.
[3] Lertratanakul A, Wu P, Dyer AR, Kondos G, Edmundowicz D, Carr J, et al. Risk Factors in the Progression of Subclinical Atherosclerosis in Women With Systemic Lupus Erythematosus. Arthritis Care Res (Hoboken). 2014;66(8):1177–85.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (