fetching data ... 
Background: Serum ferritin correlates with disease activity and poor prognosis in patients affected by anti-MDA5 dermatomyositis (DM) and interstitial lung disease (ILD). The serum ferritin concentrations were found to be elevated with a significantly high frequency in comparison with those antibody negative. Moreover, serum concentrations of ferritin at disease onset can predict the negative prognosis of anti-MDA5 DM and are associated with 1-year mortality in those patients with ILD. Conversely, no data exist for serum ferritin in other IIM-ILD nor in IIM without ILD and, remarkably, all abovementioned studies were conducted in Asian cohorts, where East Asians are known for having higher concentrations of ferritin.
Objectives: Aim of this study is therefore to assess whether serum ferritin may be considered a specific and sensitive biomarker for IIM-ILD, as well as to assess whether it correlates with clinical, radiological, functional and routine laboratory findings. To corroborate our findings, we divided the patients into a derivation and a validation group, the latter comprised by three cohorts, two from Italy and one from India.
Methods: All patients affected by IIM and followed at Siena (Italy), Palermo (Italy), Bari (Italy) and Lucknow, (India) IIM referral centers were retrospectively included. Inclusion criteria were a definite diagnosis of IIM, the availability of a definite core set measures, and serum ferritin concentrations at the first assessment (T0). Exclusion criteria were a diagnosis of inclusion body myositis and the presence of conditions directly associated with hypo or hyperferritinemia. Primary endpoints were i) to assess whether abnormal ferritin serum levels are associated with the presence of ILD and ii) to evaluate whether high ferritin serum levels can be evidenced only in anti-MDA5 DM or also in ASS ILD. Secondary endpoints were i) to assess whether ferritin serum levels differ according to the subtype of IIM; ii) to evaluate the correlation between ferritin serum levels and LFT findings, as well as with CPK, myoglobin, age at diagnosis, disease extent and damage and the occurrence of cancer; iii) to validate a serum cut-off value of serum ferritin to support ILD diagnosis, and in particular to rule in or rule out MDA5-DM, in IIM patients.
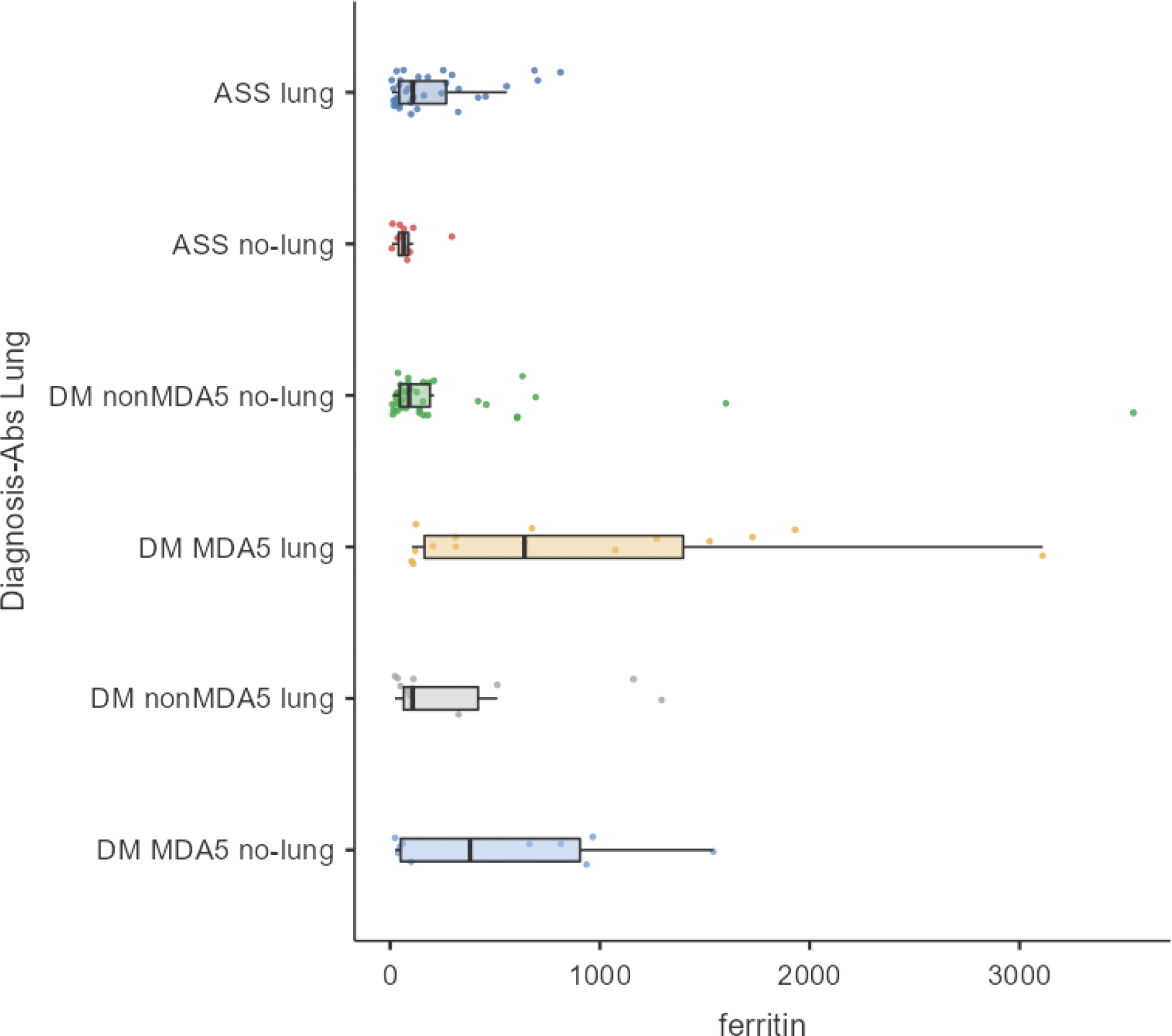
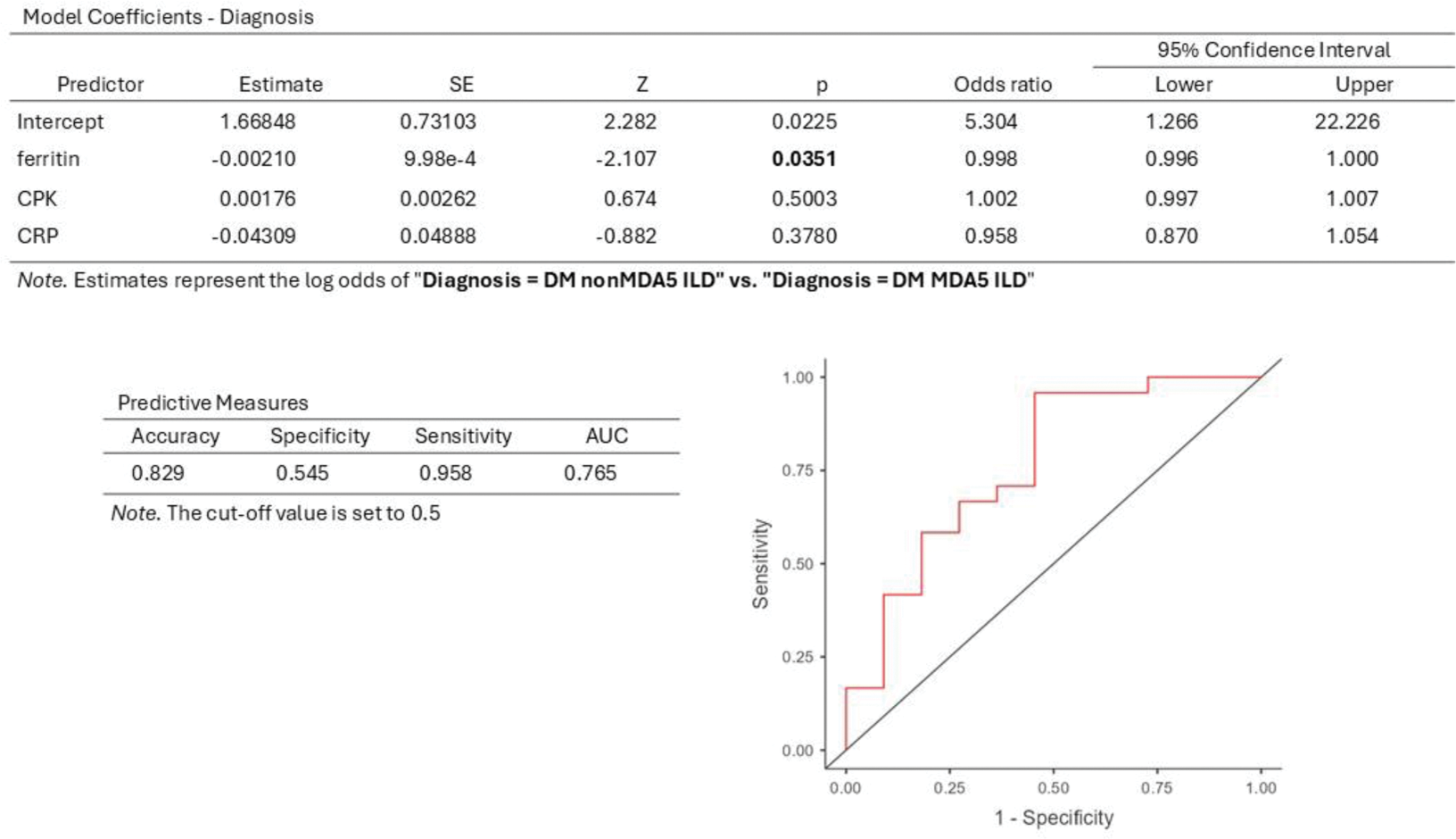
Results: A total of 139 IIM patients (51 from study and 88 from validation cohort, respectively) was included. No difference, except for age, was evidenced among the two cohorts. Stratifying patients according to their definite diagnosis (DM, PM, ASS and cancer associated myositis), no difference was found for any of the clinical, serological and lung function tests (LFT) findings. Subsequently, patients were subdivided according to their autoimmune profile and three subgroups were defined: anti-MDA5 positive DM, non-anti-MDA5 positive DM and ASS. Comparative analysis showed statistically significant difference only for ferritin (χ2 14.51; p=0.0007). Similarly, when performing pairwise comparison, anti-MDA5 DM displayed higher serum ferritin levels than ASS (W -5.28, p=0.0006) and non-anti-MDA5 DM (W -4.26, p=0.0074), while no difference was assessed between the latter. Patients were then subdivided according to the presence of ILD, showing statistically significant difference for DLCO% (p=0.00174), FVC% (p=0028), PhGA (p=0.0113), number of organs involved (p<0.0001), MDI (p=0.0001) and CRP (p=0.0067). None of the other values, including ferritin, significantly differed between the two subgroups. All 69 patients affected by ILD were subsequently divided between anti-MDA5-DM, non-anti-MDA5 DM and ASS. Comparative analysis showed statistically significant difference for ferritin (χ2 19.89; p=0.0013) (Figure 1), age at diagnosis (χ2 13.93; p=0.0161), number of organs involved (χ2 29.26; p<0.0001) and MDI (χ2 21.33; p=0.0007). ROC curve analysis of serum ferritin was performed in order to distinguish ASS and MDA5-DM with ILD obtaining a significant (p=0.0114) AUROC (0.6895) with the best cut-off value of 303.5 (sensitivity 52%, specificity 76.32%, likelihood ratio (LR) 2.196). The same cut-off (303.5 ng/ml) with higher sensitivity (66.67%) and comparable specificity was found comparing Jo1-ILD and MDA5-ILD (AUROC 0.7667, p=0.0065, LR 2.444). Even a lower cut-off (192 ng/ml) was found when comparing MDA5-ILD with all non-MDA5 ILD (sensitivity 57.5%, specificity 73.33%, LR 2.156, AUROC 0.7667). Binomial logistic regression (Figure 2) was performed to model the effect of ferritin, CRP and CPK on ILD in the two groups MDA5 and non-MDA5. Serum ferritin was independently associated with DM MDA5-ILD (p=0.0351).
Conclusion: In our study, conducted on a large, multicentric, international cohort, we evidenced that serum ferritin is not only a reliable biomarker for the early detection of ILD in case of anti-MDA5 DM, but can also distinguish these patients from ASS-ILD. In particular, a cut-off of 303.5 ng/ml seems to present a good specificity and sensitivity: in other words, when evaluating for the first time a patient with suspected IIM and ILD, waiting for autoimmunity tests, ferritin serum values lower than 303.5 ng/ml reasonably allow to exclude MDA5-DM.
REFERENCES: NIL.
Serum ferritin according to clinical diagnosis.
Acknowledgements: NIL.
Disclosure of Interests: Edoardo Conticini GSK, Eli Lilly, Dr schar, Chiesi, Latika Gupta: None declared, Marco Fornaro: None declared, Chiara Rizzo: None declared, Vikas Agarwal: None declared, Anamika Kumari Anuja: None declared, Federica Camarda: None declared, Paolo Cameli: None declared, Miriana d’Alessandro: None declared, Lidia La Barbera: None declared, Lekshmi Minikumari Rahulan: None declared, Silvia Grazzini: None declared, Stefano Stano: None declared, Giuliana Guggino: None declared, Florenzo Iannone: None declared, Elena Bargagli: None declared, Luca Cantarini: None declared, Bruno Frediani: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (