fetching data ... 
Background: Geniculate artery embolization (GAE) has gained prominence as a minimally invasive, effective intervention for chronic knee pain, particularly in osteoarthritis patients. Inspired by its success, this study explores the feasibility and efficacy of embolization for refractory pain in the first metatarsophalangeal joint (MTPJ, a frequent site of debilitating discomfort in rheumatologic practice.
Objectives: To evaluate the efficacy and safety of a novel complementary approach integrating rheumatology and interventional radiology expertise, utilizing embolization as an alternative adjunctive treatment for MTPJ pain unresponsive or refractory to conventional therapies.
Methods: Patients with chronic MTPJ pain with diverse etiologies were enrolled. Pre-procedural radiographs assessed bony structures, joint space narrowing, and signs of osteoarthritis (Figure 1a and 2a). Following local anesthesia with 2% prilocaine, vascular access was established using the Seldinger technique via the common femoral artery with 4F vascular sheath in antegrade approach. Prior to imaging, patients received 3000 IU of heparin sodium. The procedure began with roadmap imaging using a 0.035-inch hydrophilic soft guidewire and a 4F vertebral catheter to access the anterior tibial artery through the popliteal artery. Angiographic imaging identified hypervascularity in the first MTPJ, and superselective catheterization of the dorsal metatarsophalangeal artery was achieved using a 1.8 F microcatheter and a 0.014-inch guidewire. Embolization was performed using an imipenem/cilastatin suspension, administered in incremental doses of 0.5 mL until hypervascular blush resolved, while preserving distal vascular patency. Steps of the procedure were demonstrated in Figure 1b-c-d and 2b-c-d. Hemostasis was achieved by manual compression of the femoral puncture site for 15 minutes, and patients were observed in the recovery unit for six hours. All patients were discharged on the same day in the absence of complications. Clinical parameters, including Visual Analog Scale (VAS) scores, functional disability, and weekly analgesic use, were documented pre-procedure and at 4 weeks post-procedure.
Results: Seventeen feet from 13 patients (1 male, 12 females; and 12 right, 5 left feet) with a median age of 62 years (range: 41–74) underwent embolization. Diagnoses included gout (n=4), seronegative rheumatoid arthritis (n=4), spondyloarthritis (n=3), and hallux valgus with osteoarthritis (n=2). The median follow-up duration was 7 weeks (range:6–12 weeks). Significant reductions in pain and disability were observed, with both median VAS and functional disability scores decreasing from 9 (range: 5–10) to 1 (range: 0–6, p<0.0001). Weekly analgesic requirements dropped from a median of 7 (range: 3–14) to 0 (range: 0–2, p<0.0001). Successful catheterization and embolization of at least one feeder artery were achieved in all cases. One patient (5.9%) experienced transient skin discoloration, which resolved within 2 hours. No other complications were reported during the procedure or follow-up.
Conclusion: Imipenem/cilastatin-based embolization offers a minimally invasive, effective alternative for managing refractory MTPJ pain of various etiologies. The technique demonstrates significant improvements in pain relief and functional outcomes, with a favorable safety profile compared to surgical interventions. Future studies involving larger cohorts, multi-center settings, and long-term follow-up are needed to validate its safety, efficacy, and sustained clinical benefits.
REFERENCES: NIL.
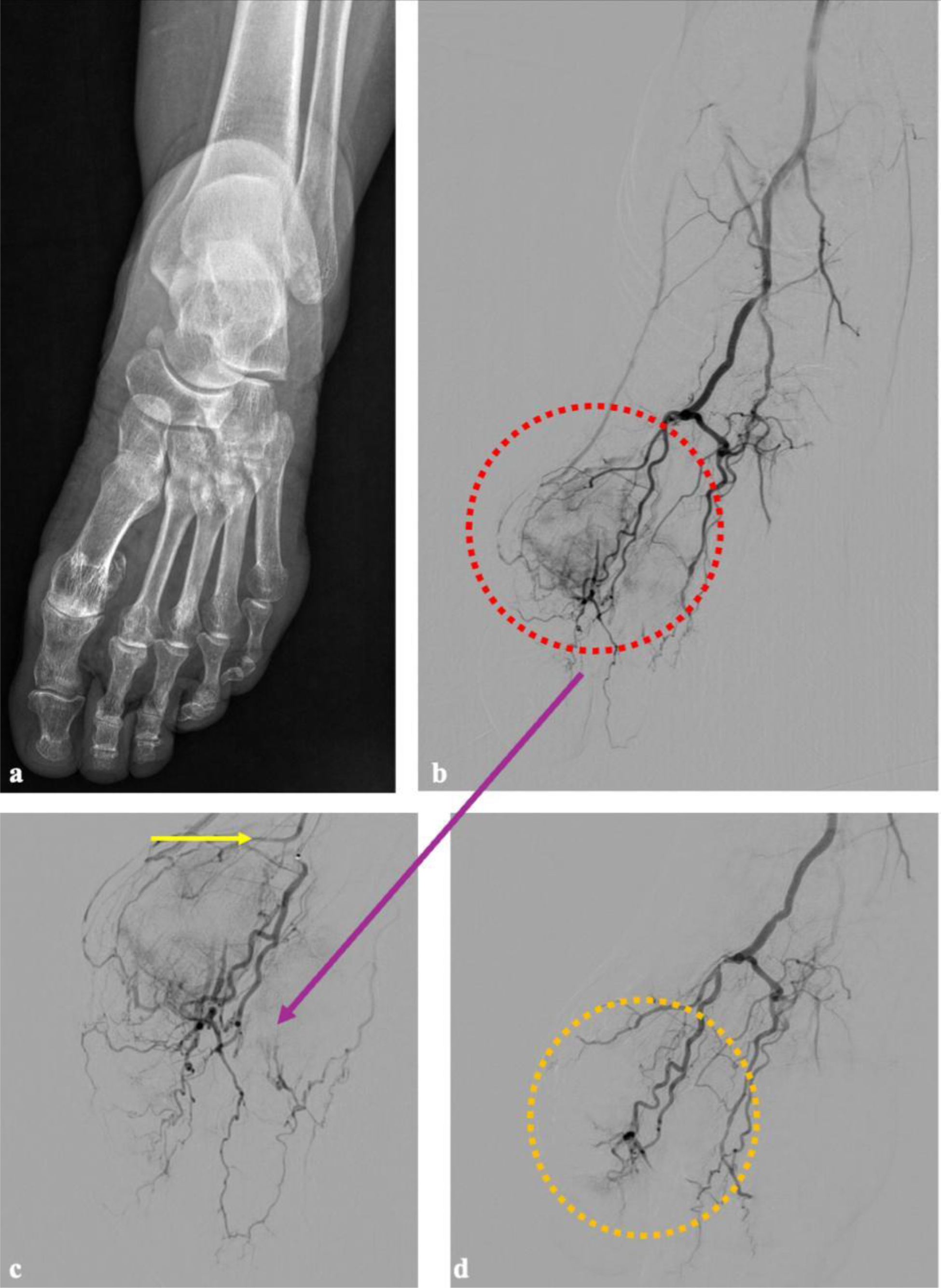
Preporcedure radiographic and procedural angiographic images of a patient with left foot embolization. In image (a) a plain radiograph image of the patient with underlying gout and narrowing in joint space suggesting osteoarthritis is given. The first procedure image (b) represents a subtracted DSA view of the entire left foot, obtained by injecting contrast through the A. dorsalis pedis. The image (c) is a non-subtracted (mask-less) angiographic view of the same region. In both images, a significant vascular blush is observed at the level of the first metatarsophalangeal joint of the left foot, followed by an enhanced appearance of venous structures due to increased inflammation. After the first dorsal metatarsophalangeal artery was superselectively catheterized using a microcatheter (c), the resulting image demonstrates a more prominent vascular blush and increased visualization of venous structures. Following superselective catheterization and embolization with imipenem/cilastatin, the blush is observed to disappear while preserving the distal vascular structures in image (d).
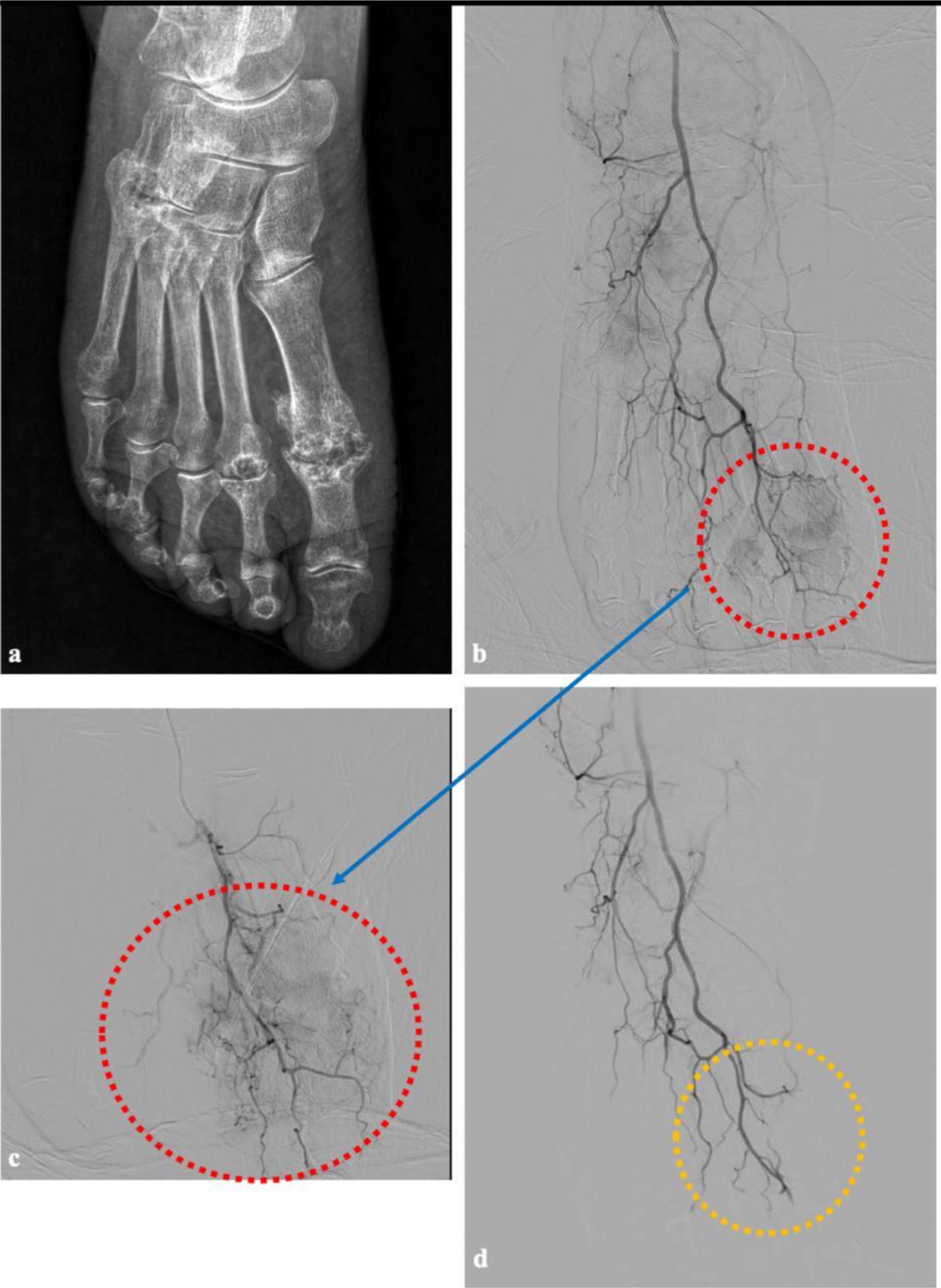
Preporcedure radiographic and procedural angiographic images of a patient with right foot embolization. In image (a) a plain radiograph image of the patient with underlying seronegative rheumatoid arthritis and narrowing in both metatarsophalangeal and tarsometatarsal joints suggesting secondary osteoarthritis is given. The first procedure image (b) represents a subtracted DSA view of the entire right foot, obtained by injecting contrast through the A. dorsalis pedis via macrocatheteraziation. The image (c) is the appearance of the first dorsal metatarsophalangeal artery after superselectively catheterizaiton using a microcatheter (c), the resulting an image demonstrating a more prominent vascular blush and increased visualization of venous structures. In image (d), following superselective catheterization and embolization with imipenem/cilastatin, macrocathetarization image shows the vascularization of the entire foot and disappearance of the blush with the while preservation of distal vascular structures.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (