fetching data ... 
Background: Achieving low disease activity state (LLDAS) within 12 months following remission induction therapy in severe systemic lupus erythematosus (SLE) has been reported to be associated with reduced risk of subsequent flares for three years [1]. However, the association between longer-term outcomes and initial, early disease control of SLE remains insufficiently understood.
Objectives: This study aimed to elucidate the impact of achieving LLDAS within 12 months after induction therapy on the long-term outcomes of patients with SLE.
Methods: We reviewed consecutive patients with severely active SLE who initiated remission induction therapy between 2015 and 2017, defined as with a British Isles Lupus Assessment Group 2004 index of A ≥1 or B ≥2, or for severe flare based on the Safety of Estrogens in Lupus Erythematosus National Assessment-SLE Disease Activity Index (SELENA-SLEDAI). Of them, we enrolled patients who were followed for 7 years and analysed the relationship between LLDAS achievement within 12 months after induction therapy initiation and long-term outcomes, including subsequent flare rates, DORIS remission status, and the Systemic Lupus International Collaborating Clinics/ American College of Rheumatology damage index (SDI) at 7 years.
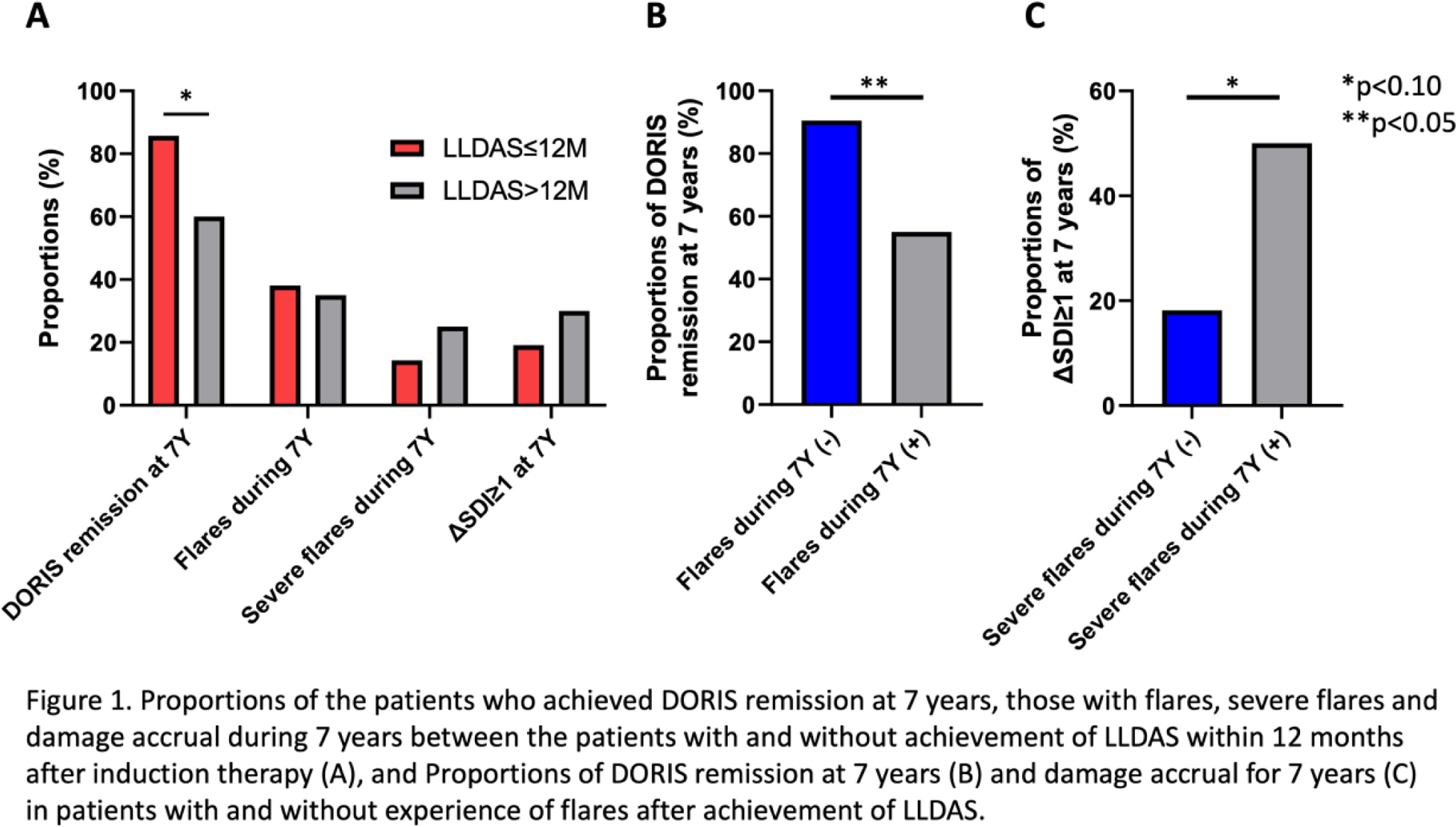
Results: Among severe SLE patients who underwent remission induction therapy, 41 patients were followed for more than seven years. The mean age was 41.6 years, with a mean disease duration of 8.2 years at the starting of remission induction therapy. The proportion of new-onset patients was 34.1%, and the mean SLEDAI score was 17.5. Renal involvement was present in 78.0% of patients. During remission induction therapy, the average starting dosage of prednisolone (PSL) was 50.7 mg/day, with 58.3% receiving cyclophosphamide, 25.0% mycophenolate mofetil (MMF), and 13.9% calcineurin inhibitors (CNI). The subsequent therapies included MMF (53.7%), azathioprine (39.0%), CNI (36.6%), and biological agents (2.4%). LLDAS was achieved within 12 months in 51.2% of patients. Over 7 years, flare and severe flare rates were 48.8% and 22.0%, respectively. The DORIS remission rate at 7 years was 73.2%, with damage accrual (ΔSDI≥1) observed in 24.4% of patients. Patients who achieved LLDAS within 12 months exhibited a trend toward a higher DORIS remission rate compared to those who did not (85.7% [n=18] vs 60.0% [n=12], p=0.086), whereas no significant differences were found in flare and severe flare rates or damage accrual (p=0.719 and p=0.484, respectively). Patients who experienced a flare had a significantly lower DORIS achievement rate at 7 years compared to those without flares (55.0% [n=11] vs 90.5% [n=19], p=0.015), and particularly, those who had severe flares after achieving LLDAS demonstrated a trend towards a higher rate of damage accrual compared to those without severe flares (50.0% [n=4] vs 18.2% [n=6], p=0.082).
Conclusion: Achieving LLDAS within 12 months after starting remission induction therapy in SLE patients is associated with higher DORIS remission rates at 7 years, particularly among those who remain flare-free during follow-up. Severe flares after achieving LLDAS may contribute to an increased risk of long-term damage accrual, suggesting the importance of optimal maintenance therapy, as well as induction therapy.
REFERENCES: [1] Kikuchi J, et al. Lupus low disease activity state within 12 months is associated with favourable outcomes in severely active systemic lupus erythematosus. Rheumatology (Oxford). 2022; 61: 3777-3791.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (