fetching data ... 
Background: Socioeconomic status is a known determinant of health disparities among patients with systemic lupus erythematosus (SLE). However, the specific impact of socioeconomic deprivation on health outcomes in regions with universal healthcare coverage, such as the Basque Country (Euskadi) in Spain, remains insufficiently studied. This region offers a unique setting to examine these dynamics, given its comprehensive public healthcare system, which ensures universal and free access to care.
Objectives: This study aimed to investigate the impact of socioeconomic deprivation on cardiovascular risk and damage in SLE patients within a universal healthcare setting in the Basque Country, Spain.
Methods: This observational cohort study included 293 SLE patients from Hospital Universitario Cruces followed for 5 years. Socioeconomic deprivation was assessed using the Socioeconomic Deprivation Index of Euskadi, classifying patients into quintiles (Q1 to Q5). Cardiovascular outcomes included the number of risk factors at diagnosis and at 5 years, and cardiovascular damage assessed by the SLICC Damage Index. Data were analyzed using multilevel linear regression models.
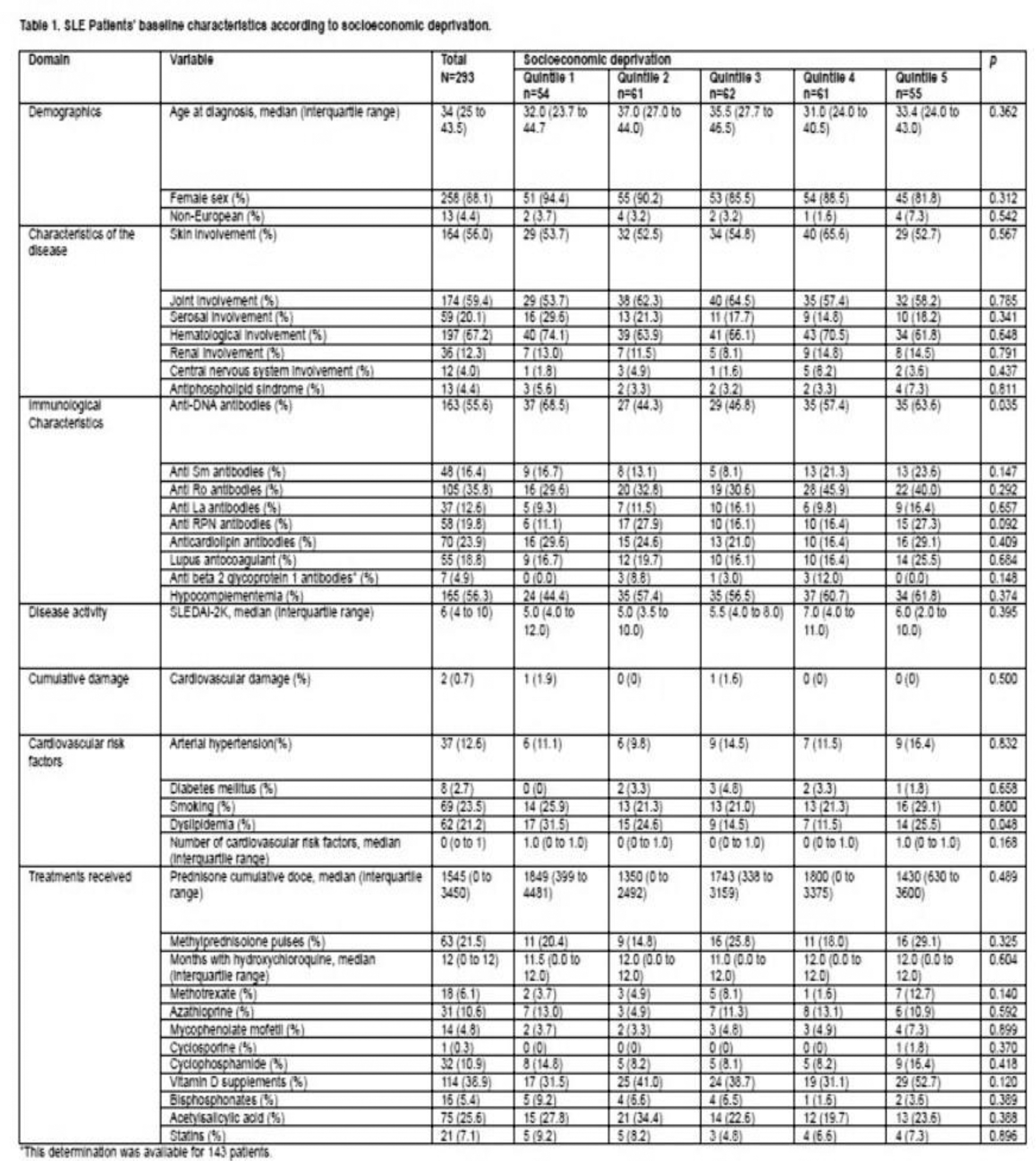
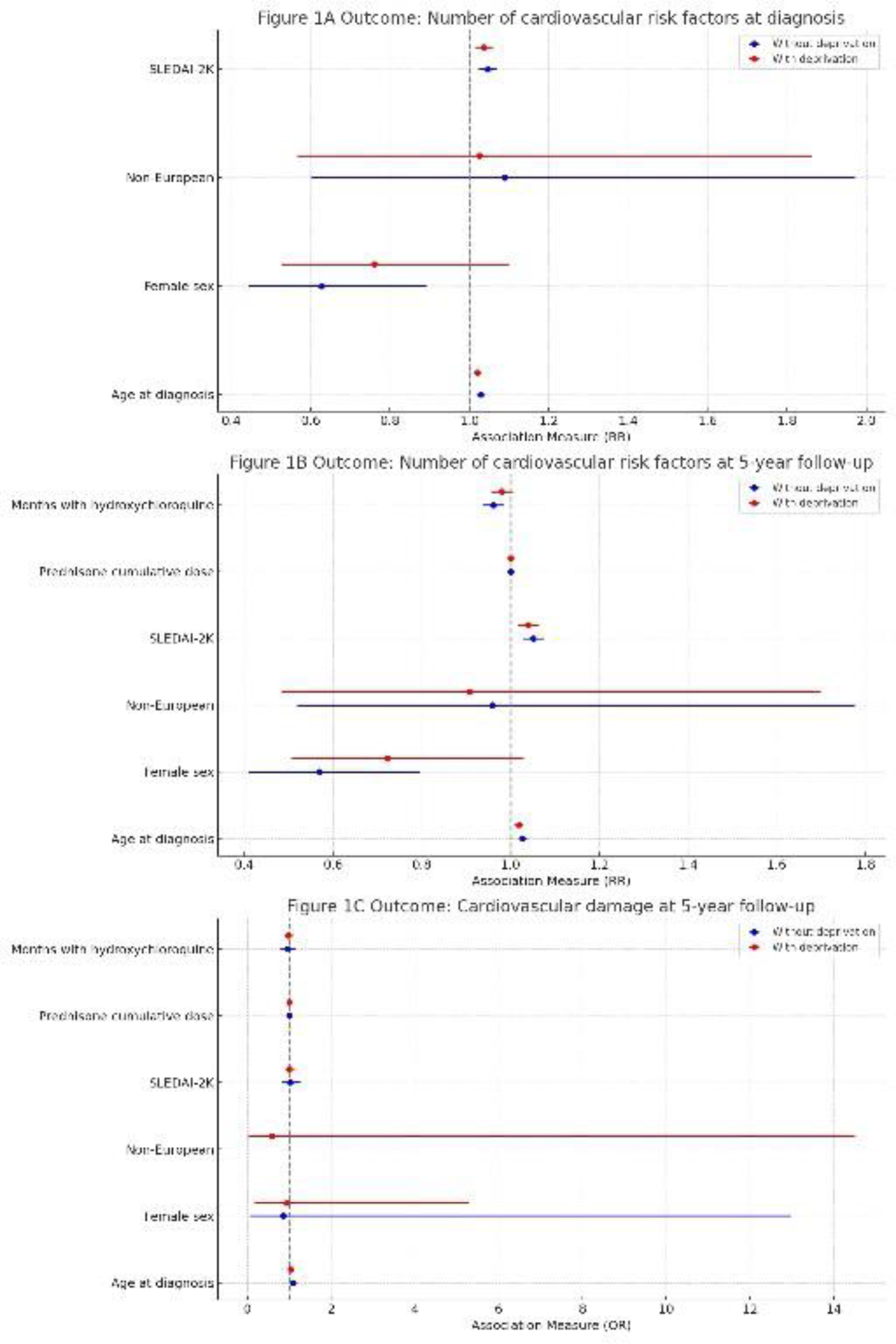
Results: Baseline characteristics showed no significant differences across deprivation quintiles, except for anti-DNA antibodies (p = 0.035) (See Table 1). The multivariate analysis shown in Figure 1 indicated no significant associations between socioeconomic deprivation and the number of cardiovascular risk factors at diagnosis (RR for Q5 vs. Q1 = 1.085, 95% CI: 0.713-1.654, p = 0.702) or at 5 years (RR for Q5 vs. Q1 = 0.977, 95% CI: 0.647-1.475, p = 0.911). No significant association was found between socioeconomic deprivation and cardiovascular damage at 5 years (OR for Q5 vs. Q1 = 1.131, 95% CI: 0.162-7.898, p = 0.901). Cardiovascular damage at diagnosis was not evaluated due to its occurrence in only two patients.
Conclusion: In this universal healthcare setting, socioeconomic deprivation was not a key determinant of cardiovascular outcomes in SLE patients. These findings suggest that equitable healthcare systems may mitigate the impact of socioeconomic disparities. Future research should explore these relationships in larger and more diverse populations to inform policies aimed at reducing health inequalities in SLE and other chronic diseases.
REFERENCES: NIL.
Acknowledgements: Dr. Ruiz-Irastorza was supported by the Department of Education of the Basque Government, research grant IT 1512-22. Dr. Hernandez-Negrin was supported by Consejería de Transformación Económica, Industria, Conocimiento y Universidades, Junta de Andalucía-Sevilla (Spain), research grant PREDOC-00826. We acknowledge ADELES Gipuzkoa and Asociación de Lupus y Autoinmunes de Castilla-La Mancha for their support. We thank Dr. Carlos Saiz-Hernando for his aid in obtaining the Socioeconomic Deprivation Index of our Lupus-Cruces patients.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (