fetching data ... 
Background: Ankylosing spondylitis (AS), also known as radiographic axial spondylarthritis (r-axSpa), is a chronic inflammatory disorder involving the axial skeleton and sacroiliac joints with age of onset usually younger than 45 years [1, 2]. The systemic inflammation associated with AS is linked to numerous negative health consequences, including accelerated atherosclerosis, increased cardiovascular mortality, and an elevated risk for comorbidities such as hypertension, metabolic syndrome and depression [3]. Data on comorbidities are valuable both for comparison between patient populations and for risk adjustment regarding associated outcomes, especially mortality. Elixhauser comorbidity index (ECI), developed in 1998, includes 30 or for some variants 31 – comorbidities, is used to predict in-hospital mortality, length of stay, adverse events and hospital discharges [4].
Objectives: We aimed to review emergency department (ED) visits, hospitalizations and discharge disposition among United States (U.S) patients with AS comparing them to patients without AS using modified ECI (29 comorbidities collected instead of 30 since rheumatoid arthritis (RA) was an exclusion criterion for this study).
Methods: Using a descriptive, retrospective, cross-sectional analysis, we analyzed ED visits and hospitalization records in the Cerner Health Facts, an electronic medical record (EMR), database from 2000 to 2017. The study included 1,575 patients with AS and 1,575 matched controls. Visits were identified if AS was listed as a diagnosis, defined by the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code: M45 at the time of admission or discharge. Patients with RA, systemic lupus erythematosus, systemic sclerosis, CREST syndrome, sjogren’s syndrome, psoriasis, crohn’s disease, ulcerative colitis, reactive arthritis, dermatomyositis, polymyositis, granulomatosis with polyangiitis, microscopic polyangiitis, eosinophilic granulomatosis with polyangiitis, giant cell arteritis, polyarteritis nodosa, and Takayasu’s arteritis were excluded from the study. Key outcomes included the ECI, diagnoses at admission or discharge, length of stay, and discharge destination. We utilized R software version 4.2.2 for statistical analysis. Patients were classified into case and control groups and Pearson’s chi-square test, Fisher’s exact test, and Wilcoxon’s rank-sum test were employed to assess significant differences for each variable across severity groups. The statistical significance was determined by using a two-sided p < 0.05.
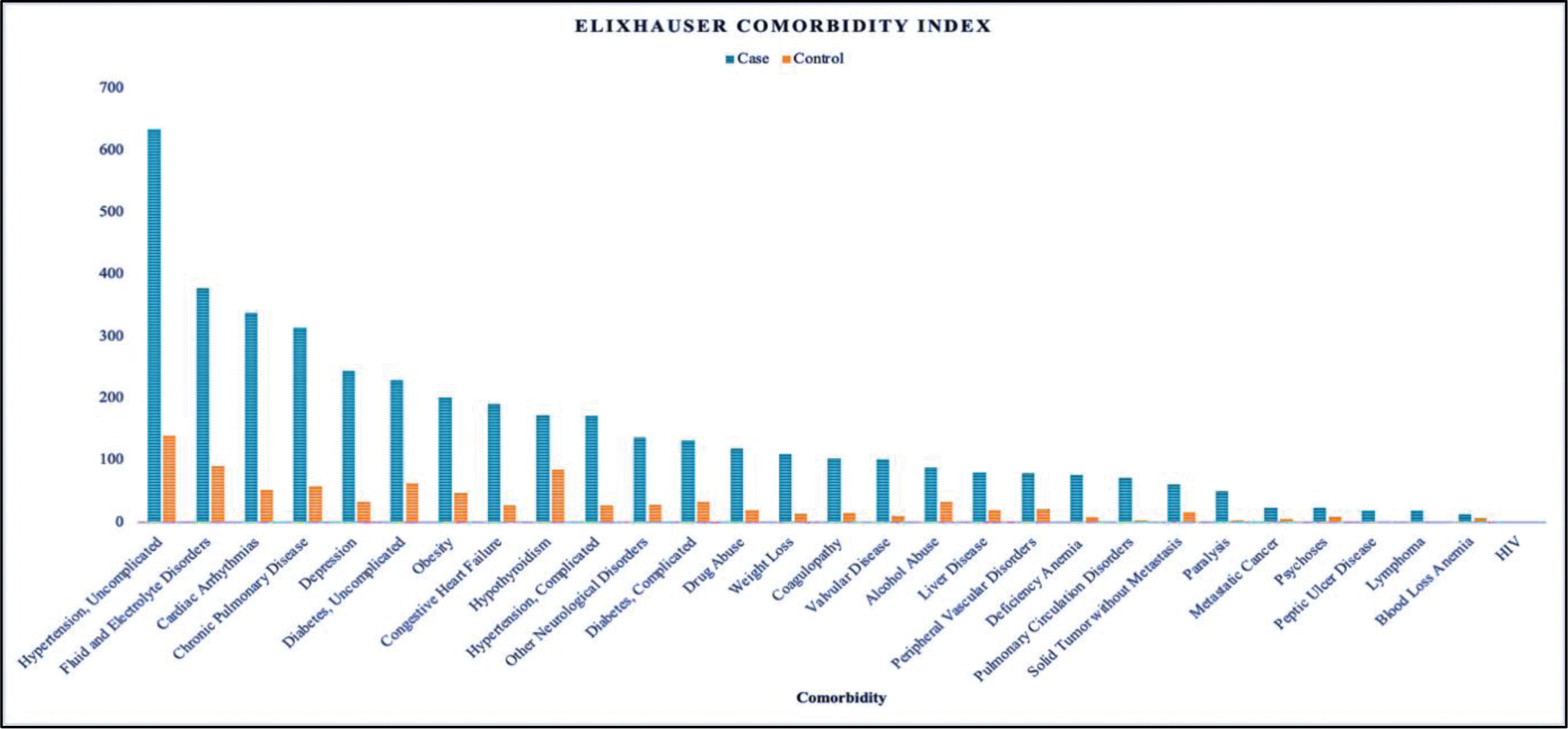
Results: There were 253 ED only visits, 964 inpatient and 130 admissions to observation among patients with a diagnosis of AS, with most cases originating from Western (35%) & Southern (34%) U.S. The visit type of 228 cases and 332 controls was unknown. Patients with AS were more likely to be admitted under inpatient or observation status (61% and 8.3%, respectively; p-value <0.001). Common diagnoses included back pain, hypertension, chest pain, and infections. Patients with AS had a higher mean ECI of 2.64 (p-value <0.001), signifying greater comorbidity burden (Figure 1), a longer average hospital stay of 11.9 days (p-value <0.001) and were more likely to be discharged to either a hospice, morgue, or rehabilitation facility (p-value <0.001) (Table 1). The study’s constraints are inherent to the nature of any retrospective database analysis. The data was collected from CERNER Health Facts without access to patient charts and was dependent on diagnosis coding by multiple providers. This introduces the potential for misclassification error, which could impact the integrity of our data. Secondly, we were limited by a lack of data on body mass index, c-reactive protein, HLA B27, tobacco use and outpatient medications.
Conclusion: Based on literature review, this is the first study of U.S patients with AS to specifically examine ED visits, length of stay, discharge destination, and ECI. As demonstrated, this study showed that patients with AS had increased risk of mortality, experienced longer hospital stays and incurred higher direct healthcare costs compared to their matched controls.
REFERENCES: [1] Van der Heijde D, Molto A, Ramiro S, et al. Goodbye to the term “ankylosing spondylitis”, hello “axial spondyloarthritis”: time to embrace the ASAS-defined nomenclature. Ann Rheum Dis . 2024;83(5):547-549. doi:10.1136/ARD-2023-225185.
[2] Reveille JD, Weisman MH. The epidemiology of back pain, axial spondyloarthritis and HLA-B27 in the United States. Am J Med Sci . 2013;345(6):431-436. doi:10.1097/MAJ.0B013E318294457F.
[3] Haroon NN, Paterson JM, Li P, Inman RD, Haroon N. Patients with ankylosing spondylitis have increased cardiovascular and cerebrovascular mortality: A population-based study. Ann Intern Med . 2015;163(6):409-416. doi:10.7326/M14-2470.
[4] Sharma, N, Schwendimann, R, Endrich, O.
et al.
Comparing Charlson and Elixhauser comorbidity indices with different weightings to predict in-hospital mortality: an analysis of national inpatient data.
BMC Health Serv Res
21
, 13 (2021).
Graphical Representation of Elixhauser Comorbidity Index
Characteristics of Patients with AS & Matched Controls
| Characteristics | Case
| Control
| p-value |
|---|---|---|---|
| Visit Type, n (% ) | <0.001 | ||
| Emergency Department | 253 (16.06%) | 843 (53.52%) | |
| Inpatient | 964 (61.20%) | 333 (21.14%) | |
| Observation | 130 (8.25%) | 67 (4.25%) | |
| Unknown | 228 (14.47%) | 332 (21.07%) | |
| Length of Stay, in Days, n (% ) | 11.9 (75.1%) | 3.1 (40.6) | <0.001 |
| Discharge Destination, n (% ) | <0.001 | ||
| Home | 1,003 (64%) | 1,010 (64%) | |
| Hospice | 61 (3.9%) | 30 (1.9%) | |
| Morgue | 32 (2.0%) | 12 (0.8%) | |
| Rehab | 189 (12%) | 66 (4.2%) | |
| Other | 290 (18%) | 457 (29%) |
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (