fetching data ... 
Background: The U1 small nuclear ribonucleoprotein particle (snRNP) is one of five snRNPs constituting the mammalian spliceosome. Its unique structural features, such as RNA-binding motifs, B and T-cell epitopes, and a distinct stimulatory RNA molecule, render it particularly vulnerable to autoimmune targeting [1]. Anti-U1 snRNPantibodies are typically associated with mixed connective tissue disease (MCTD) but are also observed in systemic lupus erythematosus (SLE), systemic sclerosis (SSc), and inflammatory myositis (IIM). The clinical relevance of these autoantibodies remains a topic of ongoing research. Key questions persist regarding the pathogenicity of anti-RNP antibodies, the specific clinical manifestations driven by the anti-RNP immune response, and the underlying mechanisms leading to anti-RNP autoimmunity . While these antibodies are commonly present alongside other autoantibodies, isolated anti-U1 snRNP positivity —defined as the presence of anti-U1 snRNP without accompanying specific autoantibodies for SLE, SSc, or other autoimmune conditions—represents a rare and distinct clinical entity. Existing literature on isolated anti-U1 snRNP positivity remains limited, with most studies focusing on its occurrence within broader autoimmune disorders. However, emerging evidence suggests that isolated anti-U1 snRNP positivity may exhibit a unique clinical phenotype.
Objectives: To delineate the clinical phenotype of patients with isolated anti-U1 snRNP positivity in an Indian population treated at a tertiary care center.
Methods: A cross-sectional observational study was conducted at Institute of rheumatology, Madras Medical College, Chennai, India, enrolled patients with isolated anti-U1 snRNP between January 2022 and December 2025. Participants: Patients with only isolated anti-U1 snRNP positivity confirmed by immunoblotting or ELISA were included. The presence of any other autoantibodies along with U1snRNP antibodies (Abs) were not included. Isolated anti-U1snRNP patients with incomplete records and pregnant women were excluded. Data Collection: A structured proforma was used to collect demographic data, clinical features, laboratory results, imaging findings and followed up. Serological testing included ELISA tests for testing ACPA, anticardiolipin and beta-2 glycoprotein Abs, RF was tested by nephelometry and ANA immunoblot assay is used to detect other antibodies such as U1RNP, Sm, dsDNA, Nucleosome, Histone, Ribosomal P, SSA Ro 52, SSA Ro 60, SSB La, Scl-70, CENP-B, Ku, PM Scl, Jo-1, Mi-2, AMA M2, PCNA. Imaging studies included HRCT chest for ILD evaluation and echocardiography screening for pulmonary artery hypertension evaluation. Nailfold video capillaroscopy is done using capillaroscope with INSPECTIS version 6.2. Statistical Analysis: Descriptive statistics were employed and analysis was performed using JASP software.
Workflow diagram.
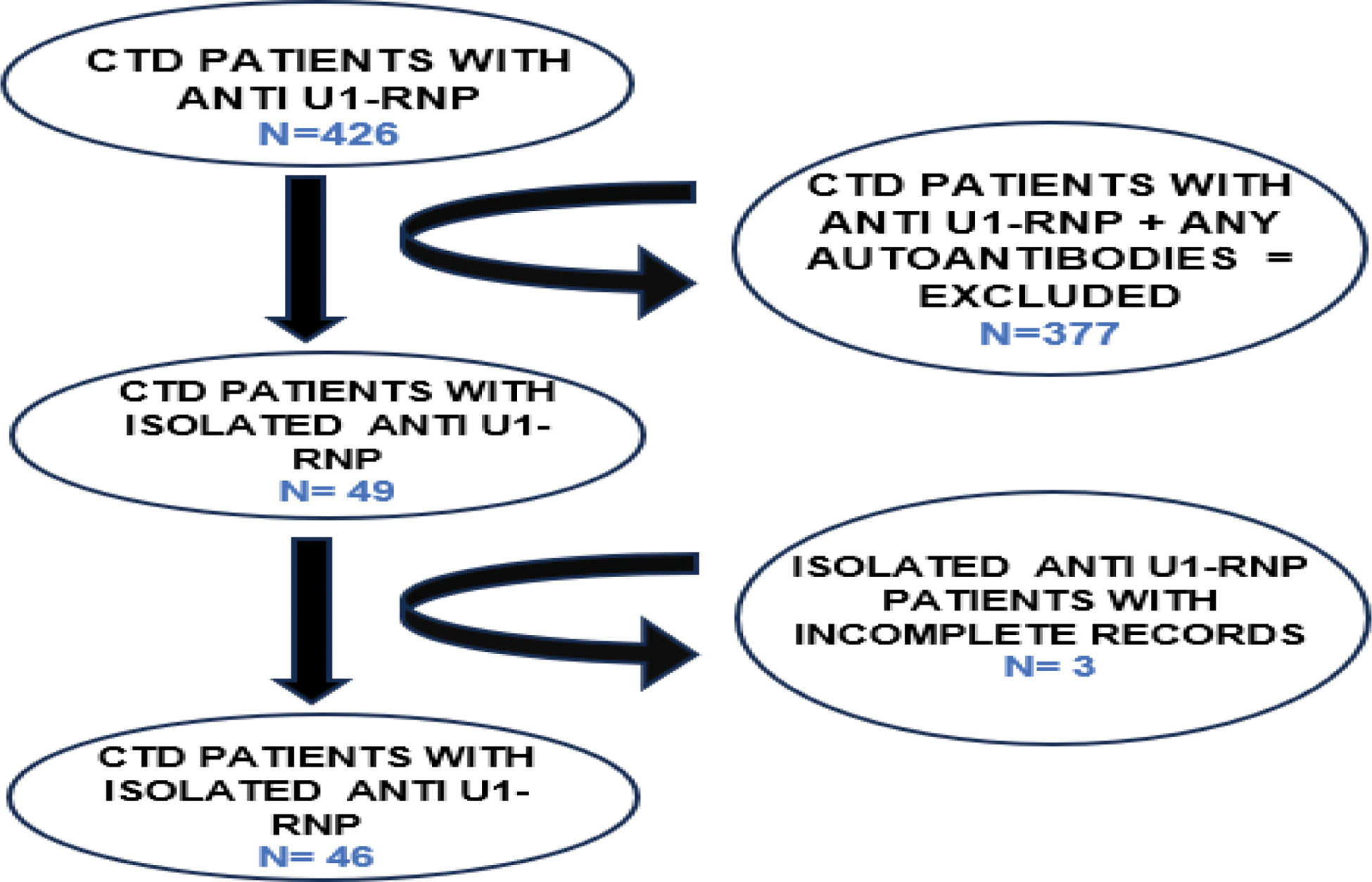
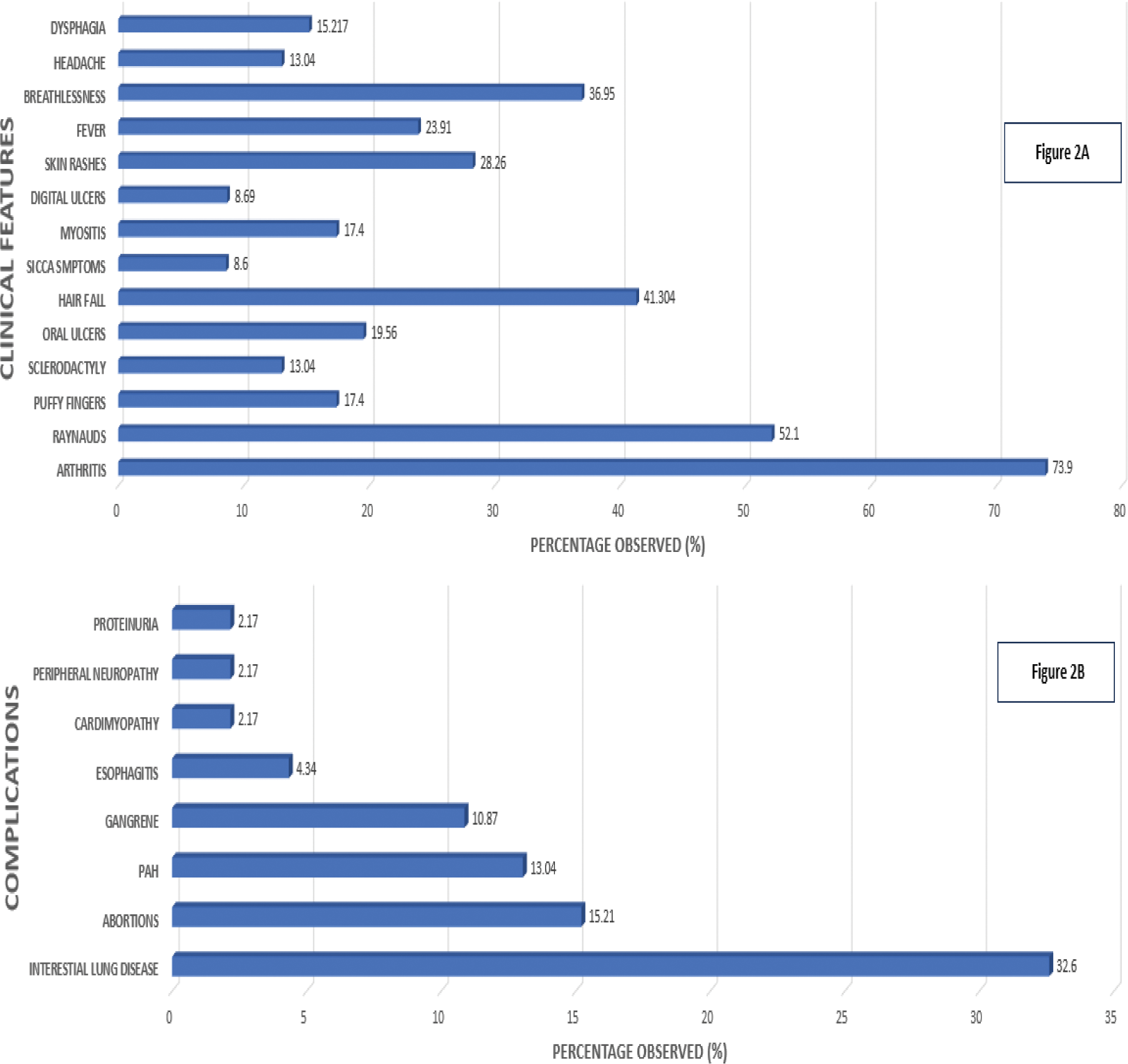
Results: Among 426 CTD patients tested positive for u1RNP, 49 had isolated U1RNP, met inclusion criteria, 3 had incomplete records were excluded and 46 patients were studied (Figure 1). The observed mean age was 35.34 ± 9.68 years. Out of 46 patients, 43 were females and 3 were males. The mean disease duration among females was 44.65 ± 33.96 months and among males was 56 ± 30.19 months. Among 43 females, 3 were unmarried and the rest were married. Among the 46 isolated u1RNP patients, 35 were diagnosed with undifferentiated connective tissue disorder (UCTD), 7 with MCTD, three with limited SSc, and one with Interstitial pneumonia with autoimmune features (IPAF). The most common clinical symptoms observed were arthritis (73.9%), Raynaud’s phenomenon (52.1 %). The rest of the clinical symptoms were summarised in Figure 2A. The most common complications observed were interstitial lung disease (32.6%) and abortions (15.21%). The rest of the complications observed were summarised in Figure 2B. Among 46 Isolated U1RNP patients, 15 patients had ILD with the NSIP pattern being predominant (66.6%) and UIP pattern in 26.6% and Early ILD in 6.67%. Out of 7 spontaneous abortions 5 were in 1st-trimester, two each in second and third-trimesters. One patient had 2 induced abortions because of binders phenotype with chondrodysplasia punctata in subsequent pregnancies. Nailfold Capillaroscopy showed a predominantly nonspecific pattern (43.47%) followed by a normal pattern (28.26%). Other patterns observed were Late systemic sclerosis (SSc) was 15.21 percent, Early SSc pattern was 8.69 percent and Active SSc pattern were 4.34 percent. Even though extensively worked up for other autoantibodies, myositis-specific antibodies are not routinely screened in all patients except mi-2 and Jo-1 antibodies.
Distribution of clinical features (2A) and complications (2B).
Conclusion: Along with other antibodies, U1snRNP Abs observed in all CTDs includes SLE, MCTD, UCTD, and SSc in varing percentage. But isolated anti-U1 snRNP positivity constitutes a distinct and rare clinical phenotype. It is characterized by arthritis and Raynaud’s phenomenon being the most common clinical feature. Interstitial lung disease, predominantly with an NSIP pattern, and first-trimester abortions emerged as the most frequent complications. Rare occurrences of congenital anomalies, such as Binder’s phenotype with chondrodysplasia punctata, as well as pulmonary artery hypertension and gangrene, were also noted. Further longitudinal studies with larger cohorts and multicentric study are essential to validate these findings and provide deeper insights into the disease’s progression and outcomes.
REFERENCES: [1] Kattah NH, Kattah MG, Utz PJ. The U1-snRNP complex: structural properties relating to autoimmune pathogenesis in rheumatic diseases. Immunological Reviews. 2010;233(1):126–45.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (