fetching data ... 
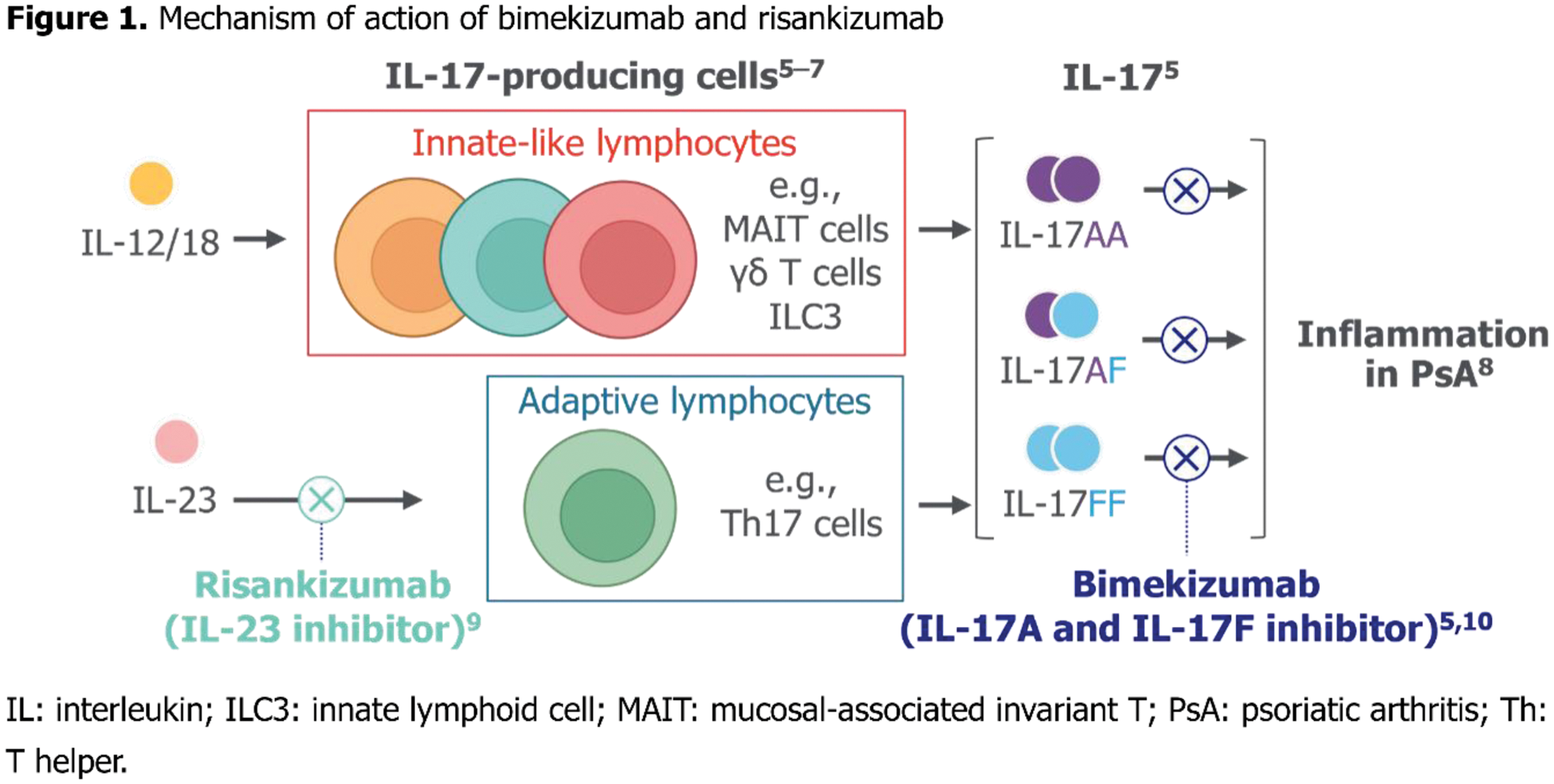
Background: Whilst there are multiple drug options for psoriatic arthritis (PsA), there is limited evidence on their comparative effectiveness and safety across clinical domains. Head-to-head studies are considered the gold standard for understanding the relative effectiveness and safety of these drugs, allowing clinicians to make informed treatment decisions. Bimekizumab, a monoclonal antibody that selectively inhibits interleukin (IL)-17A/IL-17F, has demonstrated efficacy and tolerability in PsA [1]. Risankizumab, an IL‑23 inhibitor, has demonstrated efficacy in PsA [2, 3]. IL-23-responsive cells are a significant source of IL-17A/IL-17F. However, IL-17A/IL-17F, notably IL-17F, can be produced independently of IL-23 [4]. We hypothesise bimekizumab will be superior to risankizumab in joint efficacy, by blocking IL-17A/IL-17F derived from IL-23-dependent and -independent sources (Figure 1). To test this, we present the first head-to-head study comparing efficacy and safety of bimekizumab vs risankizumab in patients with active PsA.
Objectives: To present the study design and rationale for the phase 3b BE BOLD study, including key clinical endpoints, and outline the hypothesis that bimekizumab will be superior to risankizumab in joint efficacy, by blocking IL-17A/IL-17F from both IL-23-dependent and -independent sources.
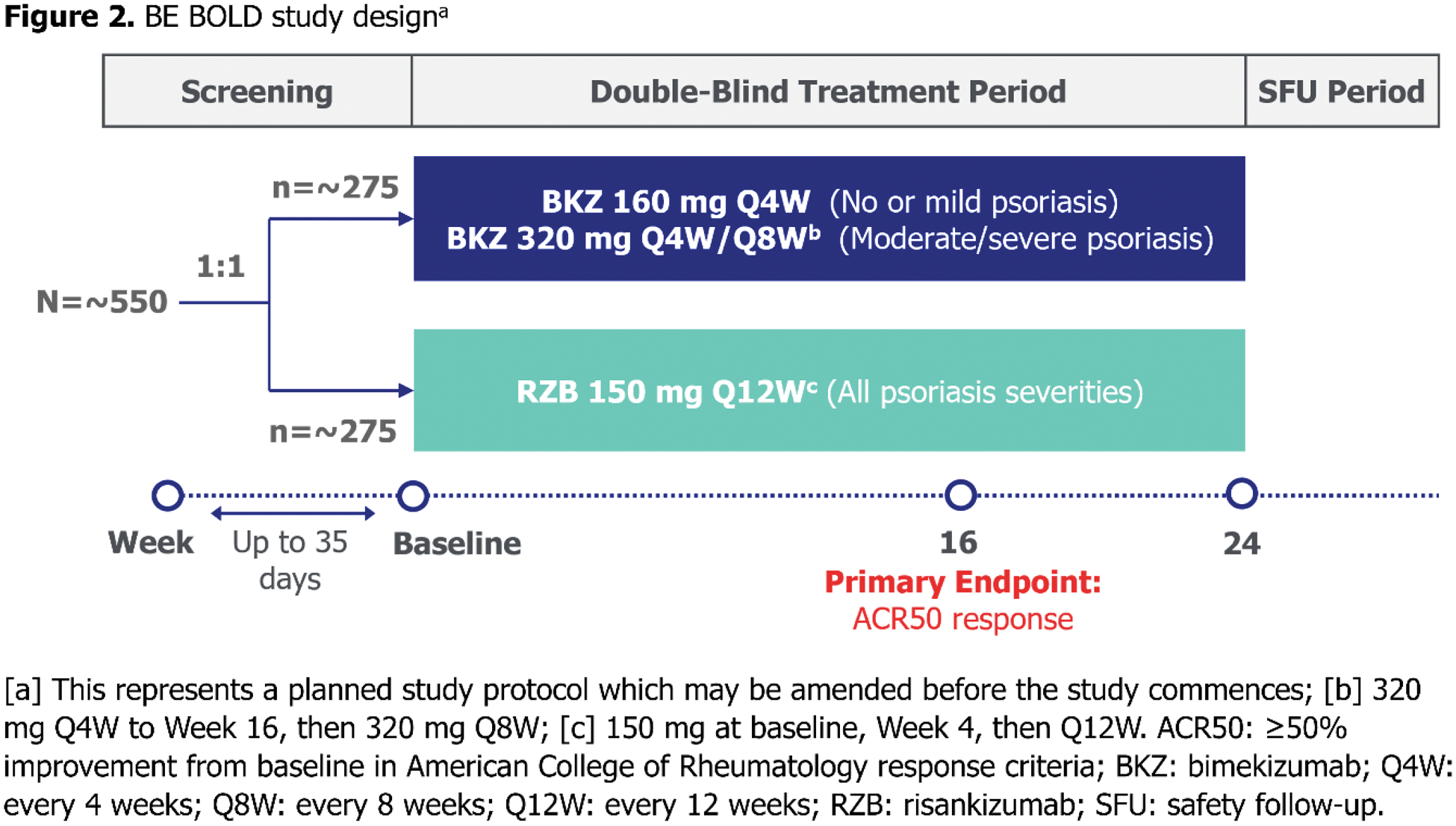
Methods: BE BOLD is a multicentre, phase 3b, randomised, double-blinded, active-controlled, parallel-group study (Figure 2). Patients with active PsA will be biologic disease-modifying antirheumatic drug-naïve or have inadequate response/intolerance to maximum one TNF inhibitor. Double-blinded period: 24 weeks. Approximately 550 patients will be randomised 1:1 to subcutaneous bimekizumab or risankizumab. Patients will be dosed according to approved bimekizumab and risankizumab labels for patients with PsA based on psoriasis severity at baseline. Psoriasis severity thresholds: no/minimal psoriasis defined as body surface area (BSA) <3%; mild psoriasis as BSA ≥3% to <10% or BSA ≥10% and either Investigator’s Global Assessment (IGA) score <3 or Psoriasis Area and Severity Index (PASI) score <12; moderate/severe psoriasis as BSA ≥10%, IGA score ≥3 and PASI score ≥12. Bimekizumab-randomised patients with none/mild psoriasis will receive subcutaneous bimekizumab 160 mg every 4 weeks (Q4W) to Week 24 with final dose of study drug at Week 20; patients with moderate/severe psoriasis will receive subcutaneous bimekizumab 320 mg Q4W to Week 16, then 320 mg Q8W. All risankizumab-randomised patients will receive subcutaneous risankizumab 150 mg at baseline, Week 4, then Week 16, regardless of baseline psoriasis severity.
Results: Primary endpoint (Week 16): American College of Rheumatology ≥50% improvement (ACR50; noninferiority/superiority vs risankizumab). Secondary endpoints: ACR50 at Week 4; Minimal Disease Activity response at Week 16; ACR50+PASI100 response at Week 16; safety outcomes (adverse events, including serious/leading to withdrawal).
Conclusion: BE BOLD is the first head-to-head study to evaluate efficacy and safety of an IL-17A/IL-17F inhibitor vs an IL-23 inhibitor in patients with active PsA; testing for superiority of bimekizumab over risankizumab in joint disease, using the primary endpoint of ACR50 at Week 16.
REFERENCES: [1] Mease PJ. Rheumatol Ther 2024;11:1363–82.
[2] Kristensen LE. Rheumatol Ther 2024;11:617–32.
[3] Östör A. Rheumatol Ther 2024;11:633–48.
[4] Navarro-Compán V. Front Immunol 2023;14:1191782.
[5] Tsukazaki H, Kaito T. Int J Mol Sci 2020;21:6401.
[6] Cole S. Front Immunol 2020;11:585134.
[7] Łukasik Z. Rheumatology (Oxford) 2021;60(Suppl 4):iv16–27.
[8] Wang EA. Eur J Rheumatol 2017;4:272–7.
[9] Pang Y. Clin Transl Sci 2024;17:e13706.
[10] Glatt S. Ann Rheum Dis 2018;77:523–32.
Acknowledgements: Funded by UCB. Editorial support provided by Costello Medical and funded by UCB.
Disclosure of Interests: Joseph F. Merola Consultant and/or investigator for AbbVie, Amgen, AstraZeneca, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, Eli Lilly and Company, Incyte, Janssen, LEO Pharma, MoonLake Immunotherapeutics, Novartis, Pfizer, Sanofi-Regeneron, Sun Pharma and UCB, Iain B. McInnes Consulting fees/honoraria from AbbVie, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Cabaletta, Causeway Therapeutics, Celgene, Evelo, Janssen, Eli Lilly and Company, MoonLake Immunotherapeutics, Novartis and UCB, Research support from Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Janssen, Novartis and UCB, Philip J. Mease Speakers bureau fees from AbbVie, Amgen, Eli Lilly and Company, Janssen, Novartis, Pfizer and UCB, Consulting fees from AbbVie, Acelyrin, Amgen, Bristol Myers Squibb, Cullinan, Eli Lilly and Company, GSK, Inmagene, Janssen, MoonLake Immunotherapeutics, Novartis, Pfizer, Takeda, UCB and Ventyx, Research grants from AbbVie, Acelyrin, Amgen, Bristol Myers Squibb, Eli Lilly and Company, Janssen, Novartis, Pfizer, Sana and UCB, Yoshiya Tanaka Speaker fees and/or honoraria from AbbVie, Asahi-kasei, Astellas, AstraZeneca, Boehringer-Ingelheim, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly and Company, Gilead, GSK, Pfizer, Taisho and UCB, Grants from Boehringer-Ingelheim, Chugai and Taisho, Alice B. Gottlieb Honoraria as an advisory board member and consultant for Amgen, AnaptysBio, Avotres Therapeutics, Boehringer Ingelheim, Bristol Myers Squibb, DICE Therapeutics, Eli Lilly and Company, Highlights Therapeutics, Janssen, Novartis, Sanofi, Teva, UCB and Xbiotech (stock options for RA), Research/educational grants from Bristol Myers Squibb, Highlights Therapeutics, Janssen and UCB (all paid to Mount Sinai School of Medicine), Akimichi Morita Speaker fees from AbbVie, Amgen, Boehringer-Ingelheim, Bristol-Myers Squibb, Eli Lilly Japan, Janssen Pharmaceutical, Kyowa Kirin, Maruho, Sun Pharma Japan, Taiho Pharmaceutical, UCB Japan, and Ushio, Consultancy fees from Amgen, Boehringer-Ingelheim, Bristol-Myers Squibb, Eli Lilly Japan, Janssen Pharmaceutical, UCB Japan, Research grants from AbbVie, Bristol-Myers Squibb, Eli Lilly Japan, Janssen Pharmaceutical, Kyowa Kirin, LEO Pharma, Maruho, Torii Pharmaceutical, and Ushio, Barbara Ink Shareholder of AbbVie, GSK and UCB, Employee of UCB, Alexander Marten Employee of UCB, Jason Coarse Shareholder of UCB, Employee of UCB, Laure Gossec Consulting fees from AbbVie, Amgen, BMS, Celltrion, Janssen, Eli Lilly and Company, MSD, Novartis, Pfizer, Stada and UCB, Research grants from AbbVie, Biogen, Eli Lilly and Company, Novartis and UCB.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (