fetching data ... 
Background: Assessing disease activity in systemic lupus erythematosus (SLE) is essential for effective treatment. SLEDAI-2K uses dichotomous items, while SLE-DAS incorporates both dichotomous and continuous variables.
Objectives: To analyze the correlation between SLEDAI-2K and SLE-DAS in SLE patients from central Spain and analyze factors leading to discordance in disease activity classification.
Methods: Retrospective assessment of 324 SLE patients followed up from 2010 to 2024 at Madrid’s Fundación Jiménez Díaz Hospital (Spain). Data were collected from the patients’ most recent visits and disease activity was evaluated using SLEDAI-2K and SLE-DAS, and discordant classifications between the tools were analyzed.
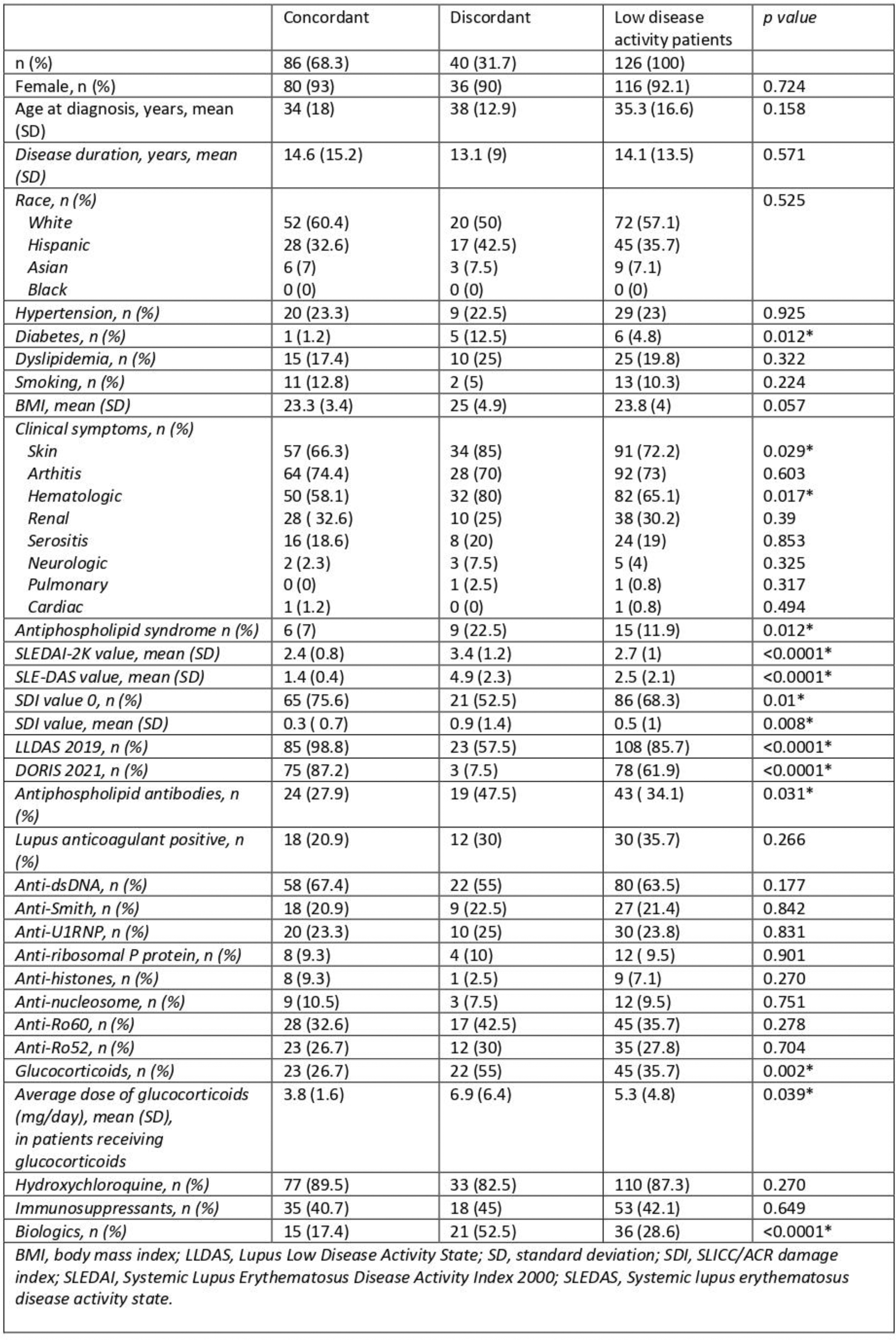
Results: The number of patients in each disease activity category was as follows: Remission (SLEDAI-2K 0, n=180 [55.6%] vs. SLE-DAS 0.37, n=180 [55.6%]); Low activity (SLEDAI 2K 1-5, n=126 [38.9%] vs. SLE-DAS ≤2.08, n=86 [26.5%]); Moderate (SLEDAI-2K 6-10, n=15 [4.6%] vs. SLE-DAS >2.08 ≤7.64, n=10 [3.1%]); Severe (SLEDAI-2K 11-19, n=3 [0.9%] vs. SLE-DAS >7.64, n=3 [0.9%]). SLEDAI-2K and SLE-DAS showed strong correlation (ρ=0.970, p<0.001), with high concordance (linearly weighted Kappa index=0.8004, p< 0.001). Forty-five patients were discordant in terms of disease activity categorization. Of these, 42 were discordant at only one level of disease activity. Notably, in 43 of the 45 discordant cases, SLE-DAS classified patients as having a higher degree of disease activity compared to SLEDAI-2K. Patients with skin and hematological manifestations were more commonly discordant in terms of disease activity (Tables 1 and 2).
Conclusion: SLEDAI-2K and SLE-DAS demonstrate a strong correlation and high reproducibility for assessing disease activity in the Spanish population. However, SLE-DAS offers additional information, particularly in patients with hematologic and skin involvement, enabling a more precise evaluation of disease activity in SLE patients.
REFERENCES: NIL.
Table 1. Clinical characteristics of 126 patients classified as having low disease activity according to SLEDAI-2K.
Multivariate analysis to identify predictors of discordant evaluation of disease activity when SLEDAI-2K and SLE-DAS were applied.
| OR CI 95% | p value | |
|---|---|---|
| Skin (ref. absence) | 4.8 (1.11-20-91) | 0.036* |
| Hematological (ref. absence) | 3.3 (0.96-11.39) | 0.059 |
| Age at diagnosis, years | 1.03 (0.99-1.07) | 0.193 |
| Glucocorticoid use (ref. no use) | 2.93 (0.86-10.04) | 0.086 |
| Biologic therapies (ref. no use) | 3.37 (0.98-11.61) | 0.054 |
| anti-sdDNA (ref. negative) | 0.34 (0.11-1.0) | 0.069 |
| Antiphospholipid syndrome (ref. absence) | 2.14 (0.41-11.18) | 0.368 |
| SDI (ref. value) | 1.41 (0.74-2.68) | 0.302 |
| LLDAS (ref. no use) | 0.01 (0.00-0.14) | <0.001* |
LLDAS, Lupus Low Disease Activity State; SDI, SLICC/ACR damage index; anti-sdDNA, anti-(double stranded)-DNA antibodies
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (