fetching data ... 
Background: Ankylosing spondylitis (AS) is a chronic inflammatory disorder that requires targeted therapies, such as TNF-α inhibitors, which are established as first-line treatments to control disease activity. However, the optimal choice of second-line therapy—whether to continue with a similar mechanism of action or switch to a different one—remains unclear.
Objectives: We aimed to evaluate the persistence of second-line targeted therapies, focusing on TNF-α and IL-17 inhibitors, using real-world data.
Methods: This nationwide study analyzed data from the National Health Insurance Database to identify incident AS cases diagnosed between 2013 and 2023. Cases were defined by at least two occurrences of the International Classification of Diseases, 10th Revision (ICD-10) code M45, along with the rare intractable disease (RID) code V140 for AS, excluding rheumatoid arthritis and systemic lupus erythematosus diagnoses. Incident AS patients treated with first-line TNF-α inhibitors followed by second-line TNF-α or IL-17 inhibitors were included. Baseline characteristics and persistence outcomes were compared between the TNF-α and IL-17 inhibitor groups. Kaplan-Meier curves and log-rank tests assessed persistence up to 12 months after initiating second-line therapy. Subgroup analyses were performed for primary non-response (prior TNF-α use <4 months) and secondary non-response (prior TNF-α use ≥4 months).
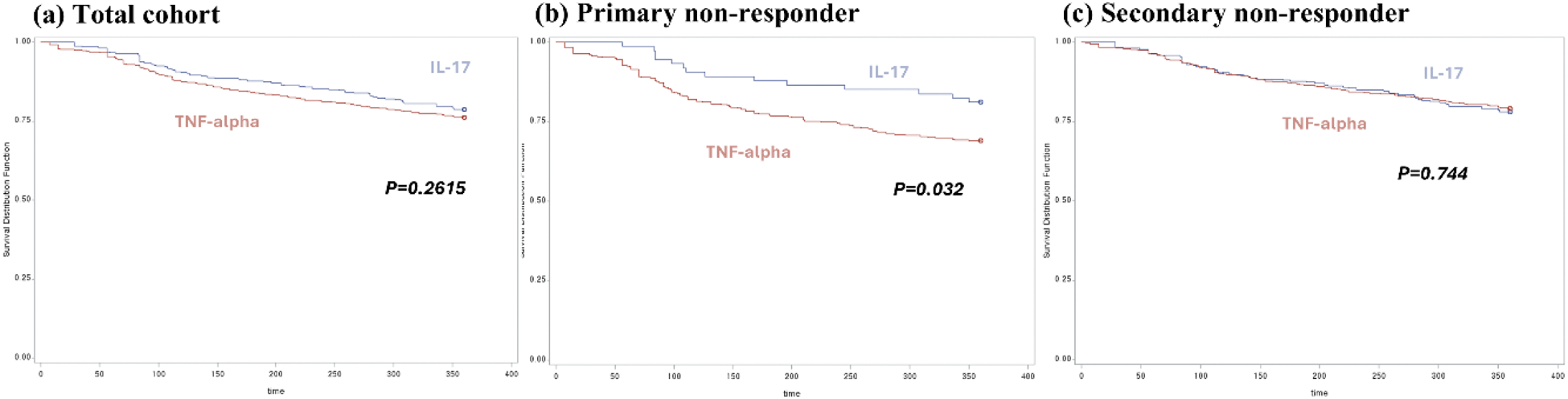
Results: A total of 1,669 patients (IL-17: 384 [23.1%], TNF-α: 1,258 [76.9%]) were included. IL-17 users were older (43.5 vs. 40.9 years; p=0.001) and more often treated in tertiary hospitals (61.2% vs. 55.4%; p=0.045). Psoriasis (21.6% vs. 6.1%; p<0.0001) and heart failure (6.5% vs. 3.2%; p=0.0034) were more prevalent among IL-17 users, while TNF-α inhibitors were more associated with uveitis (24.0% vs. 18.0%; p=0.0125). Median treatment durations were 733 days for IL-17 inhibitors and 1,015 days for TNF-α inhibitors. Retention rates at 4, 6, and 12 months showed no significant differences overall; however, IL-17 inhibitors demonstrated higher retention rates among primary non-responders (p=0.032). No significant differences were observed for secondary non-responders (p=0.744).
Conclusion: IL-17 inhibitors were more commonly prescribed to older patients, those treated in tertiary hospitals, and individuals with psoriasis or heart failure. While overall persistence was comparable, IL-17 inhibitors demonstrated better retention among primary non-responders. Further research is needed to confirm these findings.
Persistence over 12 months comparing IL-17 inhibitors and TNF-alpha inhibitors.
TNF-alpha: Tumor Necrosis Factor-alpha inhibitors; IL-17: Interleukin-17 inhibitors.
REFERENCES: NIL.
Acknowledgements: This work was supported by the Korea Health Technology R&D Project through the Patient-Doctor Shared Decision Making Research Center (PDSDM), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI23C1762).
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (