fetching data ... 
Background: Idiopathic inflammatory myopathies (IIMs) are a heterogeneous group of rare systemic autoimmune rheumatic diseases with diverse clinical manifestations affecting muscles, joints, skin, lungs, and other organs. Despite advances in treatment, the definition of remission and low disease activity (LDA) in IIMs remains inconsistent and lacks consensus, hindering accurate evaluation and comparison of therapeutic outcomes across studies.
Objectives: To conduct a scoping review of remission and LDA definitions in IIMs, addressing gaps in standardization, identifying organ-specific considerations, and examining factors positively and negatively associated with remission. An additional goal is to propose evidence-based components essential for defining remission criteria for clinical and research applications.
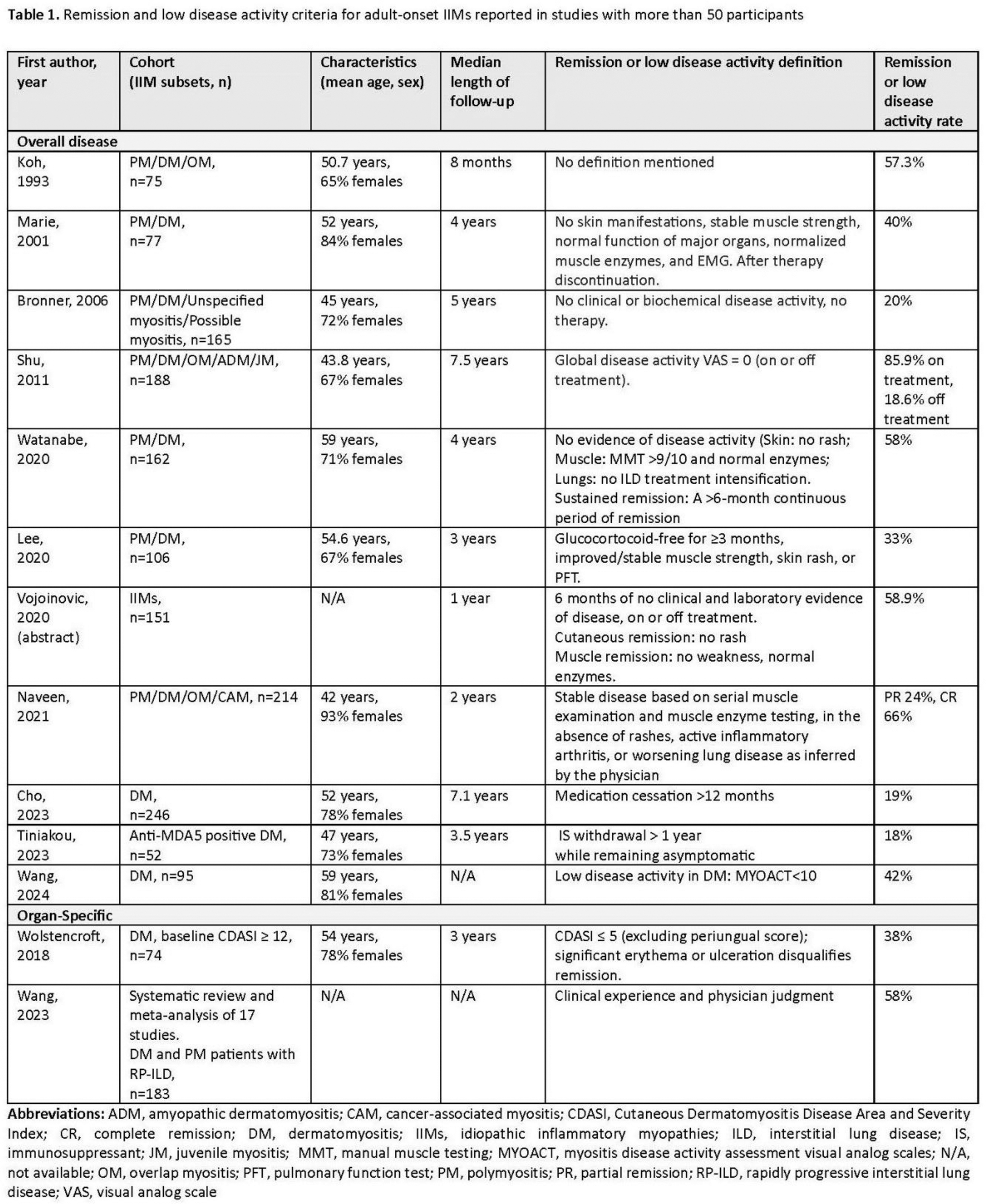
Methods: A comprehensive review was conducted by systematically searching PubMed for relevant literature on remission and LDA definitions in IIMs published up to 27 December 2024. The search strategy included a title search of “myositis” and text words of “remission”, “low disease activity”, “criteria”, and “predictors”. Bibliographies of included studies were reviewed for additional references. Studies were eligible if they were published in English, had ten or more adult participants with IIMs, and discussed remission or LDA criteria in IIMs or predictors for remission. Both natural history and interventional studies were included. Data extracted included definitions for global disease remission and LDA, definitions for organ-specific remission and LDA, identified predictors of remission, and remission rates.
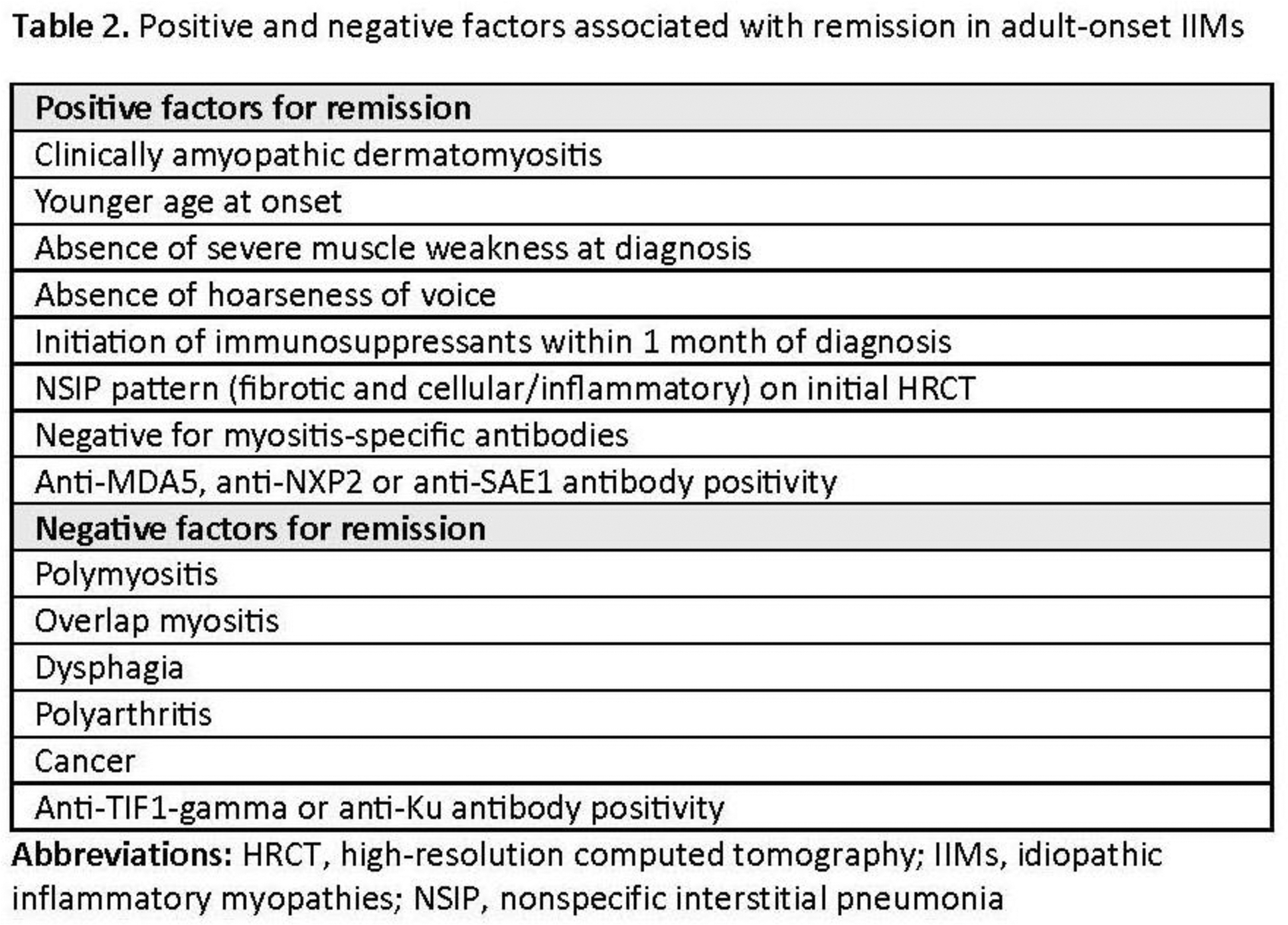
Results: Existing remission criteria for IIMs varied widely across literature, with each study’s definition primarily derived from an author-defined combination of physician assessments, laboratory normalization, imaging findings, and immunosuppressant withdrawal and/or tapering, with a typical minimum remission duration of six months. Notably, the definition of LDA was defined only in one publication as myositis disease activity assessment visual analog scales (MYOACT) of less than 10 out of 60 for the dermatomyositis subtype. Organ-specific remission was inconsistently addressed, focusing on the skin (absence of active rashes), lungs (stabilization of pulmonary function and imaging), and muscles (normal strength without biochemical evidence of activity). Reported remission rates ranged from 0% to 100%, with more stringent criteria, such as drug-free remission, yielding lower rates. Positive predictors of remission in IIMs patients included younger age, early treatment initiation, mild muscle symptoms, absence of hoarseness of voice, nonspecific interstitial pneumonia on high-resolution computed tomography, negativity for myositis-specific antibodies, and positivity for anti-MDA5, NXP-2, or SAE1 antibodies, whereas negative predictors of remission included polymyositis subtype, overlap myositis, dysphagia, polyarthritis, cancer, and positivity for anti-TIF1-gamma or Ku antibodies. Time to remission varied, with median durations ranging from 1.4 to 4 years.
Conclusion: Our scoping review confirms that published definitions for IIMs remission and LDA widely vary. The development of standardized, validated, consensus-based definitions of remission and LDA is essential to allow consistent evaluations of therapeutic outcomes in IIM. Based on our review, we propose remission should be defined as an inactive disease with a focus on key organ systems—skin, lungs, and muscles—assessed through physician evaluation, laboratory normalization, and stabilization of imaging and functional test parameters. Remission and LDA should be further categorized as either remission on therapy (stable immunosuppressive treatments) or drug-free remission. In addition, sustained remission and LDA should be defined as a continuous clinical state for 6-12 months. Establishing standardized uniform remission and LDA criteria will markedly enhance future clinical trial outcome assessments and allow improved direct comparability of treatment outcomes.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Nantakarn Pongtarakulpanit: None declared, Shiri Keret: None declared, Vaidehi Kothari: None declared, Francisca Bozan: None declared, Chengappa Kavadichanda: None declared, Akira Yoshida: None declared, Valérie Leclair: None declared, Anuradha Bishnoi: None declared, Kaveh Ardalan Cabaletta Bio, Edoardo Conticini GSK, Eli Lilly, Chiesi and Dr Schar, Ting-Yuan Lan: None declared, Océane Landon-Cardinal: None declared, Iris Yan Ki Tang: None declared, Silvia Rosina: None declared, Belina Yi: None declared, James B. Lilleker: None declared, Eduardo Dourado: None declared, Prateek C. Gandiga prior consultant honoraria from Kezar Pharmaceuticals and Jansen Pharmaceuticals, Rohit Aggarwal Octapharma, CSL Behring, Bristol-Myers Squibb, EMD Serono, Kezar, Pfizer Inc, AstraZeneca, Alexion, Argenx, Boehringer Ingelheim, Corbus, Janssen, Kyverna, Roivant, Merck, Galapagos, ActiGraph, Horizon Therapeutics, Teva, ANI Pharmaceutical, Nuvig, Capella, Cabaletta Bio, I-Cell, Sanofi, and Boehringer Ingelheim, Mallinckrodt, Pfizer Inc., Bristol Myers-Squibb, Q32, EMD Serono, Janssen, and Boehringer Ingelheim.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (