fetching data ... 
Background: Late-onset systemic lupus erythematosus (SLE) is a distinct subset of SLE characterized by onset after the age of 50. The clinical presentation, disease progression, and treatment responses may differ from younger-onset SLE.
Objectives: The aim of this descriptive study is to examine and compare the clinical features, treatment patterns, and long-term outcomes between patients with systemic lupus erythematosus (SLE) with late-onset and those with non-late-onset.
Methods: From a cohort of 516 patients, including 41 late-onset SLE cases, we applied propensity score matching to match late-onset and non-late-onset patients in a 1:3 ratio. The propensity score was calculated using sex and disease duration as matching variables. To achieve an optimal balance, Nearest Neighbor Matching was performed using a calibre of 0.05. Non-parametric variables were analysed using the Mann-Whitney U test, parametric variables with t-tests, and categorical variables with chi-square tests. The significance level was set at p < 0.05.
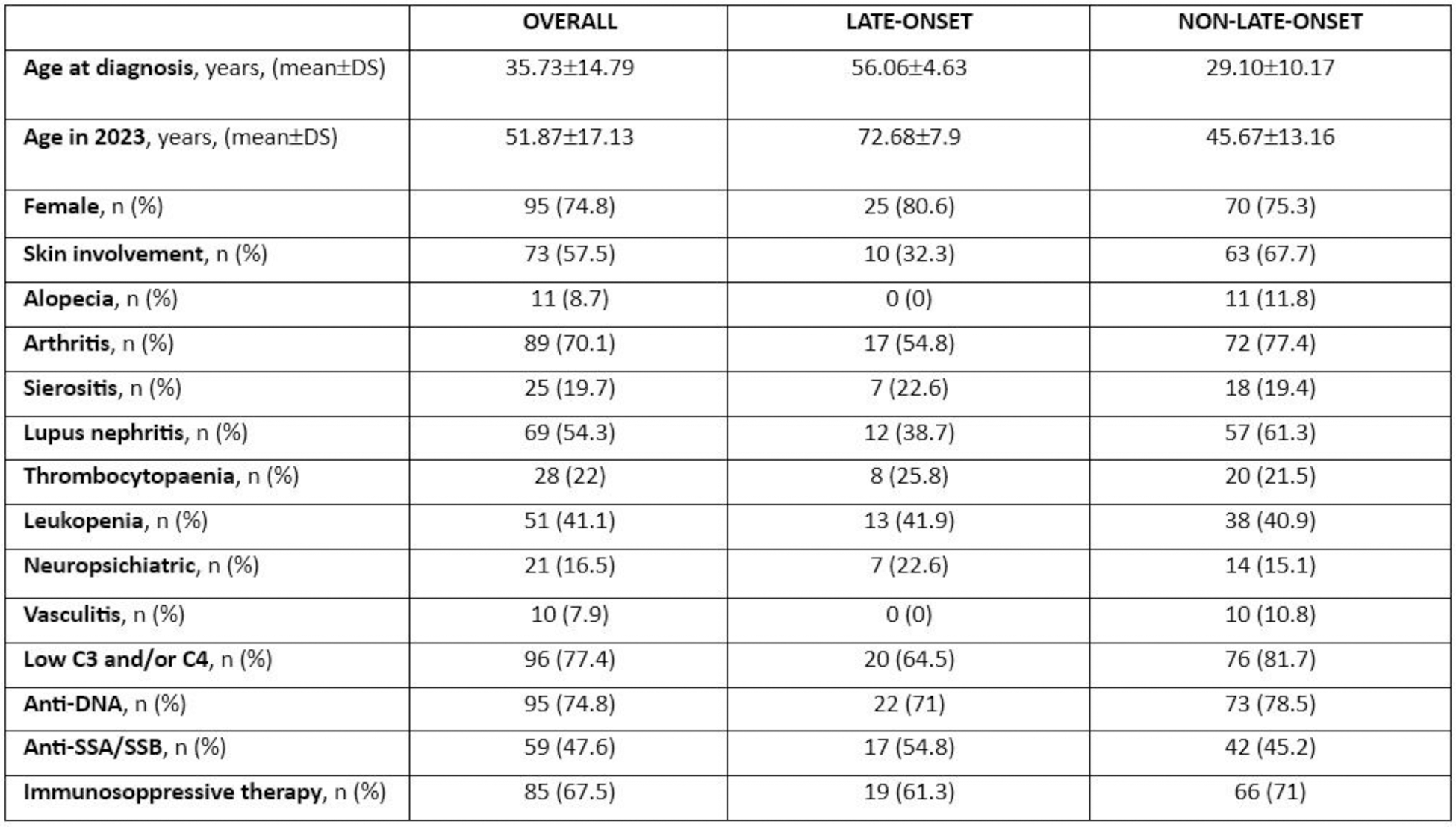
Results: After applying the propensity score, we identified 31 late-onset and 93 matched non-late-onset SLE patients. Late-onset patients exhibited a lower prevalence of arthritis (54.8% vs. 77.4% p=0.039), nephritis (38.7% vs. 61.3%, p=0.043), and cutaneous involvement (32.3% vs. 67.7%, p=0.001). Overall, during the disease course late-onset patients displayed similar patterns of disease activity compared to non-late-onset SLE patients, though they tended to have a higher prevalence of monophasic pattern (55% vs. 33%). Accordingly, no significant differences were observed in the types and number of immunosuppressive drugs used between the two groups, including rituximab and belimumab, and in the cumulative dose of glucocorticoids (GC) over the disease course (19.1 g ±12.5 vs. 17.9 g ±11.7, p=0.65). Notably, anifrolumab was used exclusively in non-late onset SLE patients (11 cases). At last follow-up, mean SLEDAI-2K was lower in late-onset SLE (1.3±1.6 vs. 2.4 ± 2.7, p=0.002), and a higher proportion of patients had a clinical SLEDAI-2K=0 (96.7% vs 76.4%, p=0.014). Despite that, at last follow-up mean steroid dose was similar (1.3 mg ±2.1 vs. 2.1 mg ±3.5, p=0.15) with equal proportions of patients being GC-free (64.5%), on low-dose GC (≤7.5 mg/day, 32.3%) and on high-dose GC (>7.5 mg/day, 3.2%). Late-onset patients exhibited a greater cumulative organ damage (median (IQR) SDI: 2 (1-3) vs. 1 (0-2), p=0.001) but a similar GC-related damage (p=0.05). Severe damage (i.e. SDI≥2) was more frequently observed in late vs. non-late-onset patients (50% vs. 22.3%, p=0.006).
Conclusion: Despite similar use of GC in terms of cumulative dose and of immunosuppressive therapies, including biologics, patients with late-onset SLE showed lower disease activity at follow-up, but higher cumulative organ damage, with a greater prevalence of severe damage. These findings highlight the need for tailored strategies to balance disease control and long-term outcomes in this population.
REFERENCES: NIL.
Table 1.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (