fetching data ... 
Background: Nailfold video capillaroscopy (NVC) is gaining importance in evaluating connective tissue diseases. However, its role in systemic lupus erythematosus (SLE), a heterogeneous disease lacking clear subclassification markers, remains undefined. Typical SLE phenotypes relate to the dominating type of organ involvement (e.g. dermatological or renal) or autoimmune serology associated with distinct manifestations (e.g. anti-phospholipid syndrome (APS)), which have revealed differences in prognosis and treatment [1]. Neuropsychiatric manifestations appear more frequently in SLE patients with APS, and recent studies have reported a significant presence of capillary dilatations in SLE patients and frequent micro-haemorrhages in those with APS [2]. These findings lend credibility to the notion that NVC may serve as a clinical tool for improving early awareness and monitoring of SLE patients with a view to reduce damage accrual. We hypothesized that NVC patterns not yet established or validated for SLE associate with said SLE phenotypes.
Objectives: Nailfold video capillaroscopy (NVC) is gaining importance in evaluating connective tissue diseases. However, its role in systemic lupus erythematosus (SLE), a heterogeneous disease lacking clear subclassification markers, remains undefined. Typical SLE phenotypes relate to the dominating type of organ involvement (e.g. dermatological or renal) or autoimmune serology associated with distinct manifestations (e.g. anti-phospholipid syndrome (APS)), which have revealed differences in prognosis and treatment [1]. Neuropsychiatric manifestations appear more frequently in SLE patients with APS, and recent studies have reported a significant presence of capillary dilatations in SLE patients and frequent micro-haemorrhages in those with APS [2]. These findings lend credibility to the notion that NVC may serve as a clinical tool for improving early awareness and monitoring of SLE patients with a view to reduce damage accrual. We hypothesized that NVC patterns not yet established or validated for SLE associate with said SLE phenotypes.
Methods: We did NVC and clinical characterization, including Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) evaluation, on 56 SLE patients. NVC was performed using a digital video-capillaroscope (x200 magnification). An experienced capillaroscopist examined all fingers except thumbs bilaterally and scored the changes on a semiquantitative scale (0,1,2,3). Correlations within NVC findings were tested using Spearman’s rho, subsets of patients with similar NVC changes were identified by hierarchical cluster analysis of principal components of Z-normalised scores, and associations with clinical phenotypes were analysed using multinomial logistic regression.
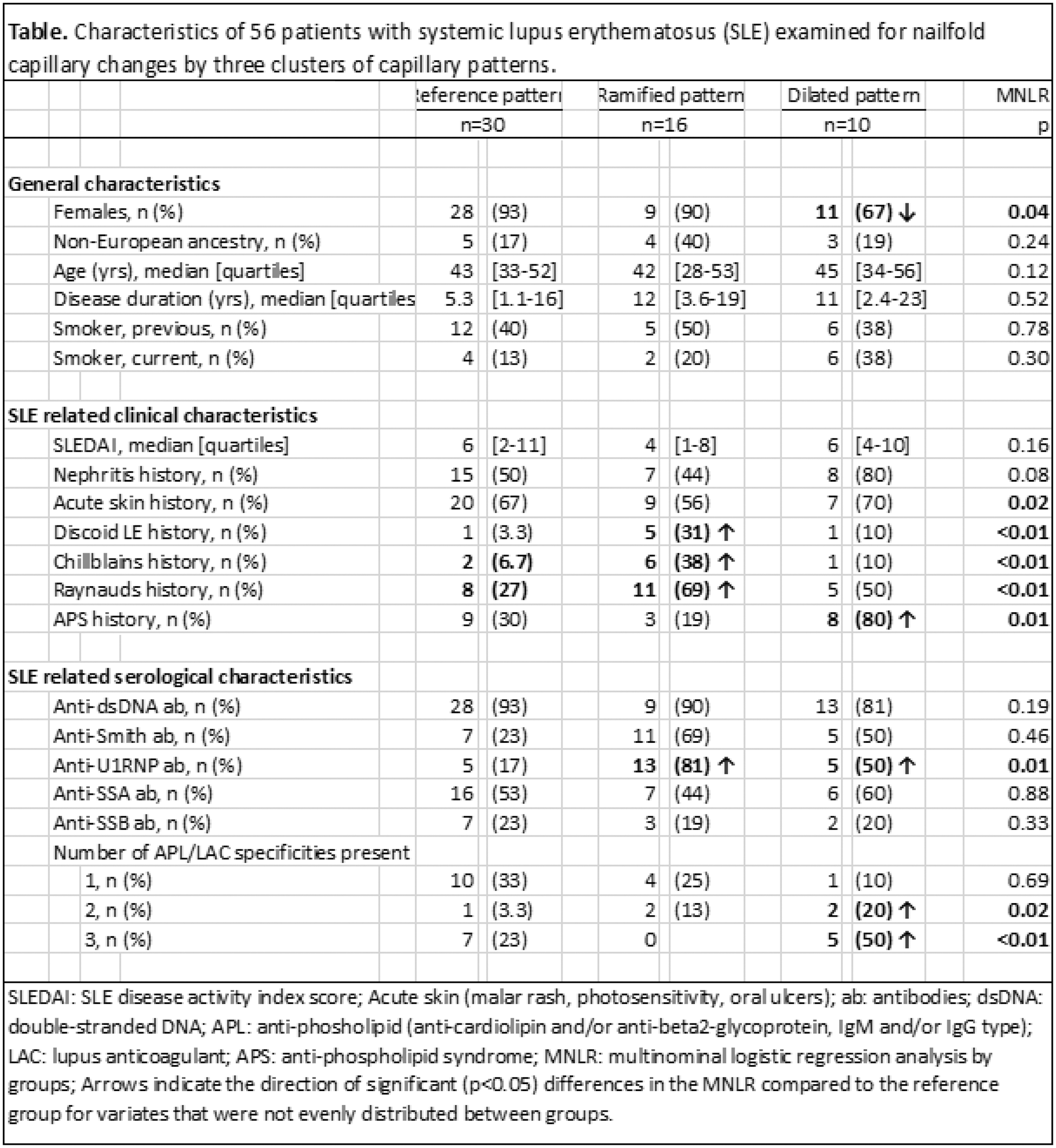
Results: The study included 56 SLE patients (85% female) with a median age of 43 years (IQR: 32-53). Clinical manifestations included nephritis (54%), acute cutaneous lupus erythematosus (54%), discoid lupus erythematosus (13%), chilblains (16%), Raynaud’s phenomenon (43%), and APS (36%). The median SLEDAI score was 6 (IQR: 3-10). Capillaroscopic alterations observed were: Ramifications (66%), disorganization (89%), tortuous appearance (75%), low density (86%), meandering appearance (52%), dilatations (23%), micro-bleedings (29%) and other irregularities (64%). Mega capillaries were not observed. Cluster analysis revealed three distinct clusters of NVC findings. One cluster was set as reference (REF, n=30), another was dominated by ramifications (RAMI, n=16), and the third was dominated by dilations (DIL, n=10), Figure 1. These clusters were associated with distinct clinical phenotypes, as shown in Table 1. Both clusters showed correlations with U1RNP antibodies. The RAMI cluster correlated with discoid lupus, chilblains, and Raynaud’s phenomenon and the DIL cluster correlated with APS and the presence of ≥2 antiphospholipid antibodies.
Conclusion: Capillaroscopic alterations are frequent in SLE patients, with capillary ramifications and dilations being associated with distinct SLE phenotypes. NVC may thus hold potential to prove useful in better risk prediction of certain organ involvements in SLE patients, however, this remains to be investigated in larger prospective cohorts using validated definitions of capillary changes relevant to SLE.
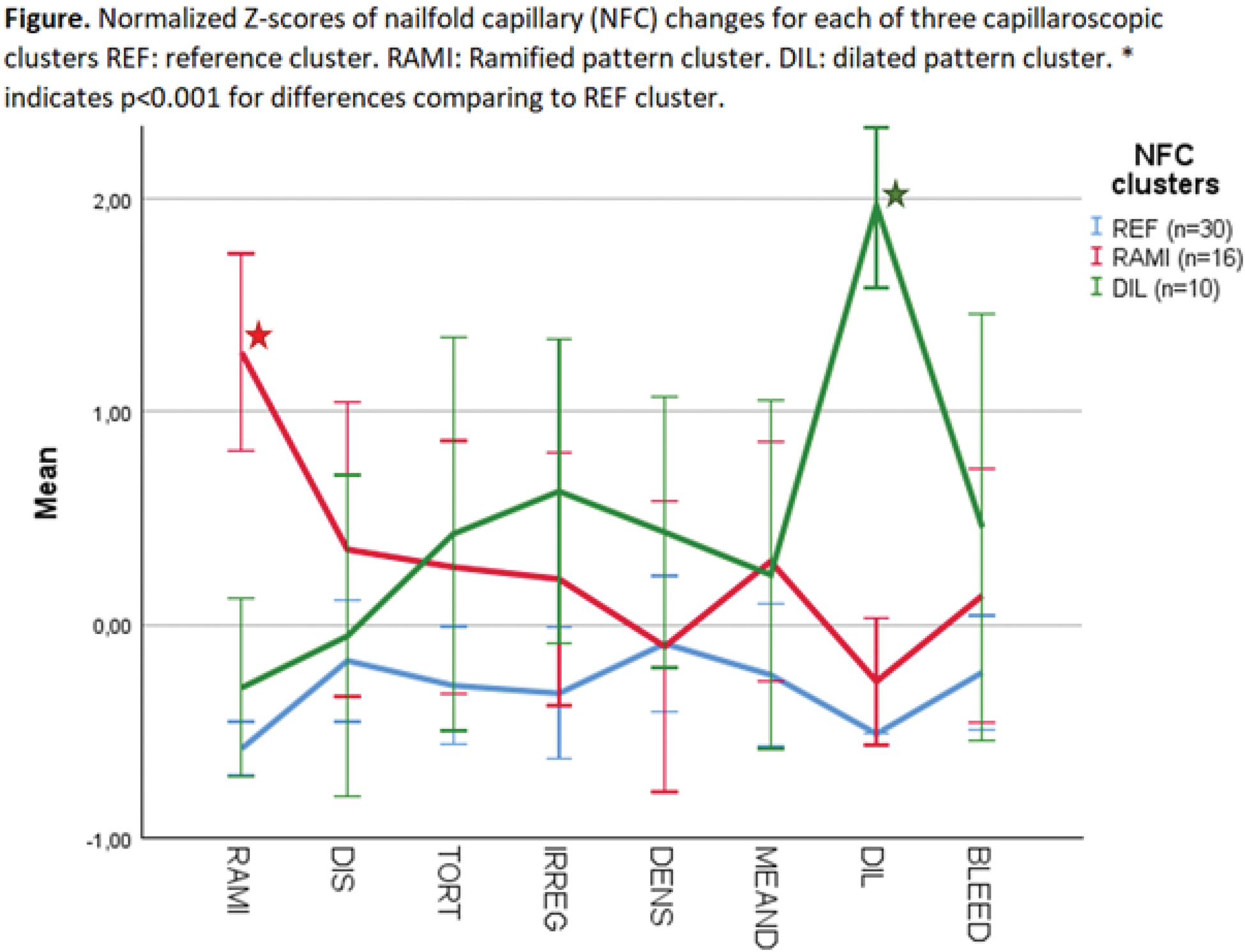
Table 1.
REFERENCES: [1] Fanouriakis, A et al., Update on the diagnosis and management of systemic lupus erythematosus. Ann Rheum Dis, 2021. 80(1):14-25.
[2] Smith, V., et al., Nailfold capillaroscopy. Best Pract Res Clin Rheumatol, 2023. 37(1):101849.
Acknowledgements: NIL.
Disclosure of Interests: Line Kjær Winberg: None declared , Mojgan Sarafrazi: None declared , Malte Lund Adamsen: None declared , Amanda Hempel Zinglersen: None declared , Henrik Leffers: None declared , Louise Pyndt Diederichsen: None declared , Søren Jacobsen Astra Zeneca, Lundbeck.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (