fetching data ... 
Background: Few studies have investigated the impact of rurality on systemic lupus erythematosus (SLE). In the GLADEL cohort, patients living in rural areas had lower socioeconomic status, lower education levels, more severe disease activity at diagnosis, and a higher rate of renal damage compared to those in urban areas [1]. Furthermore, Gergianaki et al. demonstrated that musculoskeletal and cutaneous involvement was more frequent in rural than urban patients [2].
Objectives: To evaluate the impact of rurality on the clinical presentation and outcome of a cohort of SLE patients referring to the Hub centre of our Region in Italy.
Methods: Sociodemographic, clinical, and laboratory data from a monocentric cohort of 261 SLE patients meeting the 2019 EULAR/ACR criteria were retrospectively collected. Residence was defined as rural if it met at least one of the following criteria: population density <150 inhabitants/km² or distance from the hub center > 45 km (mean distance, ie, 25 km + 1 standard deviation, ie, 20 km). The disease severity was defined according to the EULAR recommendations (3). The disease activity was assessed based on the Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) score, while damage was defined according to SLICC/ACR damage index (SDI). Comparisons between two independent groups for continuous variables were conducted using parametric and non-parametric methods, depending on the distribution of the data. Normality was assessed using the Shapiro-Wilk test, and homogeneity of variances was evaluated using Levene’s test. If the data met the assumptions of normality and homogeneity of variances, an independent samples t-test was employed. For data that did not meet the assumption of normality, the Mann-Whitney U test was used as a non-parametric alternative. For qualitative variables, comparisons between groups were performed using the Chi-square test of independence. When the expected frequency in any cell of a contingency table was less than five, Fisher’s exact test was used. All statistical analyses were performed using SPSS version 15. Statistical significance was set at p < 0.05.
Results: Ninety-six patients (36.8%) were classified as rural, with 8 (3.1%) meeting both rurality criteria (density <150 inhabitants/km² and distance > 45 km). The mean duration of disease for the entire cohort was 22,3±9 years and there were no differences between urban and rural patients, positive for 1 or 2 criteria (respectively p = 0,49 and p = 0,55). Among rural patients, no statistically significant differences were observed in major variables (disease severity, number/type of organ involvement) compared to urban patients, except for a higher tendency toward at least one renal, serositis, articular, or neurological involvement (p=0.09). Considering the 8 patients meeting both rurality criteria, we observed:
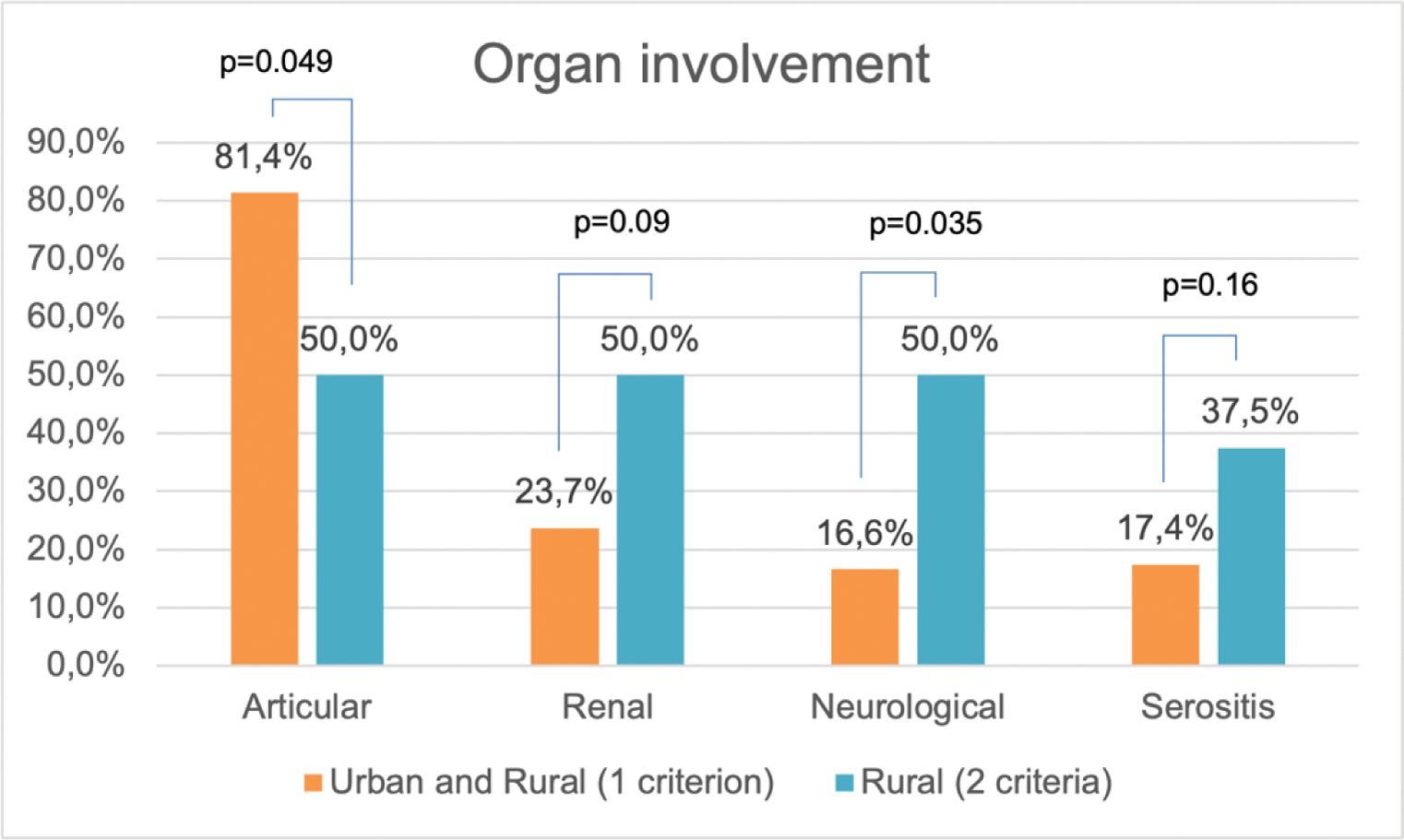
Statistically significant lower articular involvement (50% vs. 81.4%; p=0.049), and higher neurological involvement (50% vs. 16.6%; p=0.035) in rural patients (2 criteria) (Figure 1).
A trend towards increased incidence of renal (50% vs. 23.7%; p = 0.09) and serositis involvement (37.5% vs. 17.4%; p = 0.16) in rural patients (2 criteria) (Figure 1).
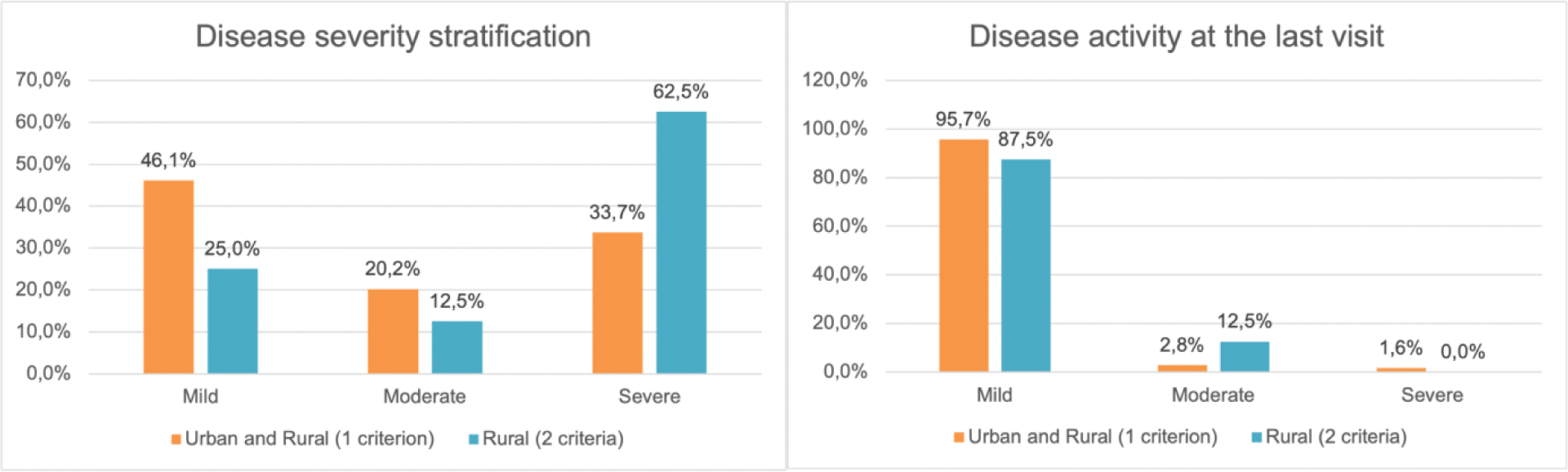
An increased frequency of severe cases among patients with both rurality criteria: mild (25% vs. 46.2%), moderate (2.5% vs. 20.2%), and severe (62.5% vs. 33.7%). However, the disease activity at the last follow-up was comparable except for moderate activity: mild (87.5% vs. 95.7%), moderate (12.5% vs. 2.8%), and severe (0% vs. 1.6%) (Figure 2).
A significant greater damage accrual among patients with both rurality criteria vs urban or rural (1 criterion) patients: median SLICC-DI [range] 1 [0-5] vs 0 [0-5], p=0.03.
Additionally, patients living in areas with a population density <150 inhabitants/km² (N = 64) seemed to have lower education levels (up to middle school) compared to those in denser areas (31.3% vs. 20.8%; p = 0.09).
Conclusion: In our cohort, geographically disadvantaged patients exhibited a globally more severe disease profile and lower educational attainment. However, long-term outcomes did not differ significantly from urban residents, likely due to the accessibility of a hub center within 45-50 km, possibly mitigating baseline sociocultural and geographical disadvantages.
REFERENCES: [1] Pons-Estel GJ, Saurit V, Alarcón GS, Hachuel L, Boggio G, Wojdyla D, et al. The impact of rural residency on the expression and outcome of systemic lupus erythematosus: data from a multiethnic Latin American cohort. Lupus. 2012 Nov;21(13):1397-404. doi: 10.1177/0961203312458465.
[2] Gergianaki I, Fanouriakis A, Adamichou C, Spyrou G, Mihalopoulos N, Kazadzis S, et al. Is systemic lupus erythematosus different in urban versus rural living environment? Data from the Cretan Lupus Epidemiology and Surveillance Registry. Lupus. 2019 Jan;28(1):104-113. doi: 10.1177/0961203318816820.
[3] Fanouriakis A, Kostopoulou M, Alunno A, Aringer M, Bajema I, Boletis JN, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019 Jun;78(6):736-745. doi: 10.1136/annrheumdis-2019-215089.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (