fetching data ... 
Background: Osteoporosis associated with fragility fractures (FF) is a significant comorbidity in patients with Systemic Lupus Erythematosus (SLE). Systemic inflammation, genetic predisposition linked to a family history of fractures, insufficient sun exposure and pharmacological management often lead to reduced bone mineral density. This phenomenon also affects patients typically at low risk for FF, such as premenopausal women.
Objectives: In this cross-sectional study, we applied cluster analysis to a large cohort of female SLE patients to identify the disease phenotype associated with FF.
Methods: For this analysis, we enrolled female patients with SLE (based on the 2019 ACR/EULAR criteria) who had undergone bone mineral density assessment using dual-energy X-ray absorptiometry (MOC DEXA) within the three months preceding their last visit. Epidemiological, anthropometric, clinical, and laboratory data were recorded, along with medication history. Chronic damage was assessed using the SLICC Damage Index (SDI). FF presence was evaluated using conventional radiology methods, and the 10-year fracture risk was estimated using the DEFRA index. An unsupervised cluster analysis for variables was conducted.
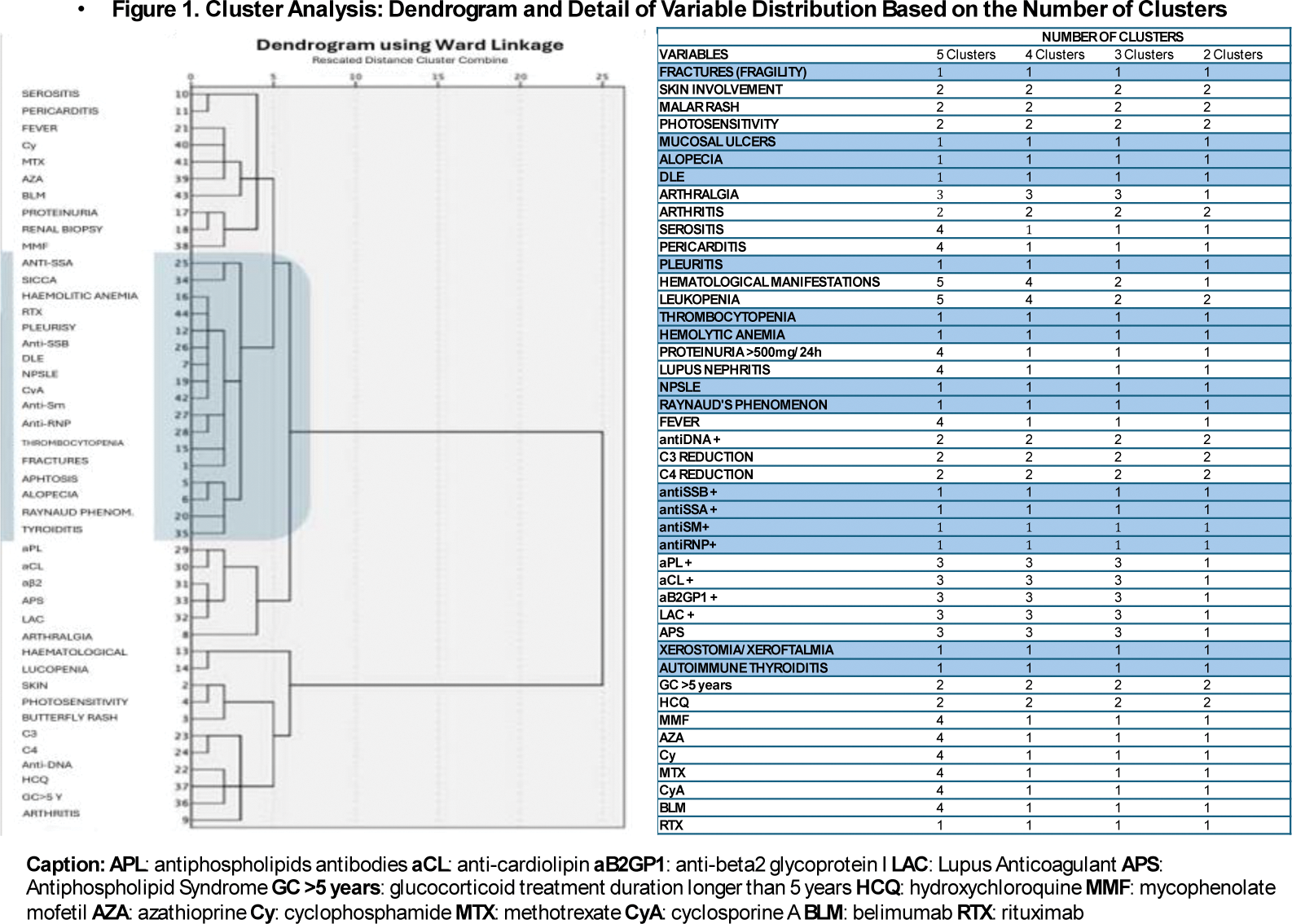
Results: We evaluated 153 women (median age 56 years, IQR 14; median disease duration 216 months, IQR 204). At the time of evaluation, 100 patients (65.3%) were postmenopausal, with a median age at menopause onset of 50.2 years (IQR 9.25). Based on MOC DEXA T-scores, 44 patients had osteoporosis (28.9%; median femoral T-score -1.6, IQR -1.45; median lumbar T-score -1.7, IQR -1.7). Radiographic evaluation identified FF in 27 patients (17.7%). Univariate analysis showed significant associations between osteoporosis and SDI≥1 (p=0.01), mucosal ulcers (p=0.03), Cyclosporine A use (p=0.02), and between FF and SDI≥1 (p=0.00004), photosensitivity (p=0.0005), and hemolytic anemia (p=0.001). According to DEFRA scores, 41.2% of patients had a 10-year fracture risk exceeding 25%. Cluster analysis (Figure 1) revealed that regardless of the number of clusters, FF was included in a specific disease phenotype characterized by thrombocytopenia, hemolytic anemia, cutaneous and neuropsychiatric manifestations, pleuritis, ENA positivity, and autoimmune thyroiditis.
Conclusion: In this study, cluster analysis identified a specific disease phenotype associated with FF. In particular, the association between FF and hematological manifestations may be attributed to the use of high doses of glucocorticoids for treating these manifestations. Furthermore, the presence of autoimmune thyroiditis in the same cluster underlines the need for a comprehensive evaluation of SLE patients, including comorbidities.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (