fetching data ... 
Background: Autoimmune rheumatic diseases predominantly affect women, especially during their reproductive years. These conditions have a substantial influence on multiple aspects of a woman’s life, with reproductive health being a critical area of concern. They encompass vital domains such as family planning, fertility, pregnancy, and obstetric outcomes. The impact of these chronic autoimmune diseases on reproductive health is significant and stems from several factors, including the presence of active disease, the use of teratogenic medications, hormonal imbalances, and various psychosocial challenges.
Objectives: To study factors influencing obstetric outcomes in women of reproductive age group with Autoimmune rheumatic diseases (AIRD).
Methods: Total of 261 cases and 272 age-matched controls participated in a questionnaire-based study to assess autoimmune and inflammatory rheumatic diseases (AIRD). Participants provided demographic information, disease type, current activity, medications, pregnancy details, and obstetric outcomes. They were categorized into six groups: Rheumatoid Arthritis (RA), Systemic Lupus Erythematosus (SLE), Spondylarthritis (SpA), Sjögren’s Syndrome (SjS), Scleroderma, and Others. Two-thirds of the patients had disease durations of less than five years. Key predictors of adverse obstetric outcomes for AIRD patients included high disease activity during pregnancy, use of teratogenic drugs, ANA positivity, Ro positivity, antiphospholipid syndrome, and maternal age over 35 years. Data was managed in Microsoft Excel and analysed using SPSS v23 (IBM Corp.), presenting descriptive statistics and performing regression analyses to assess predictors of poor obstetric outcomes. A bidirectional stepwise selection was used to determine the most significant variables for the final predictive model.
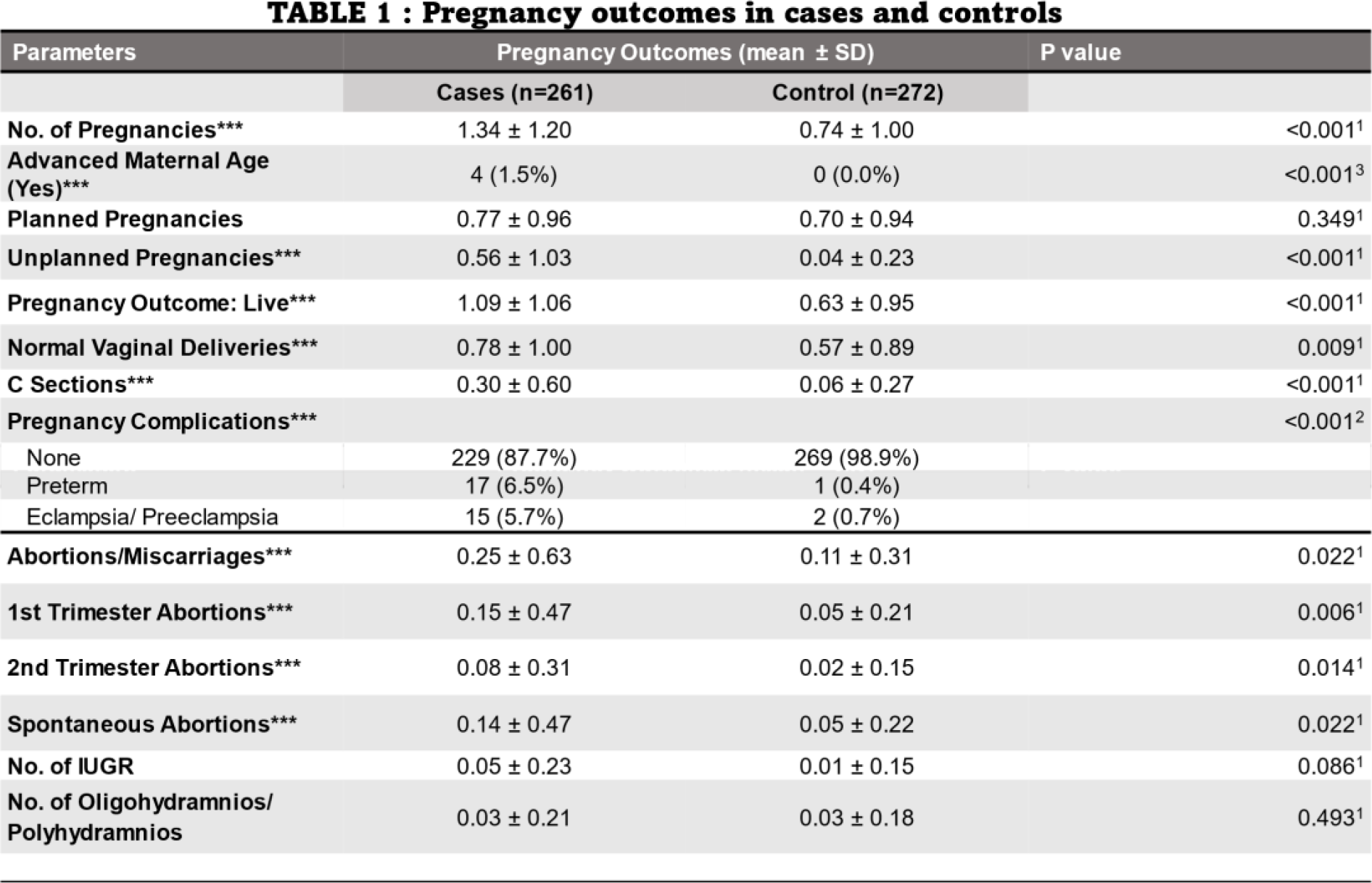
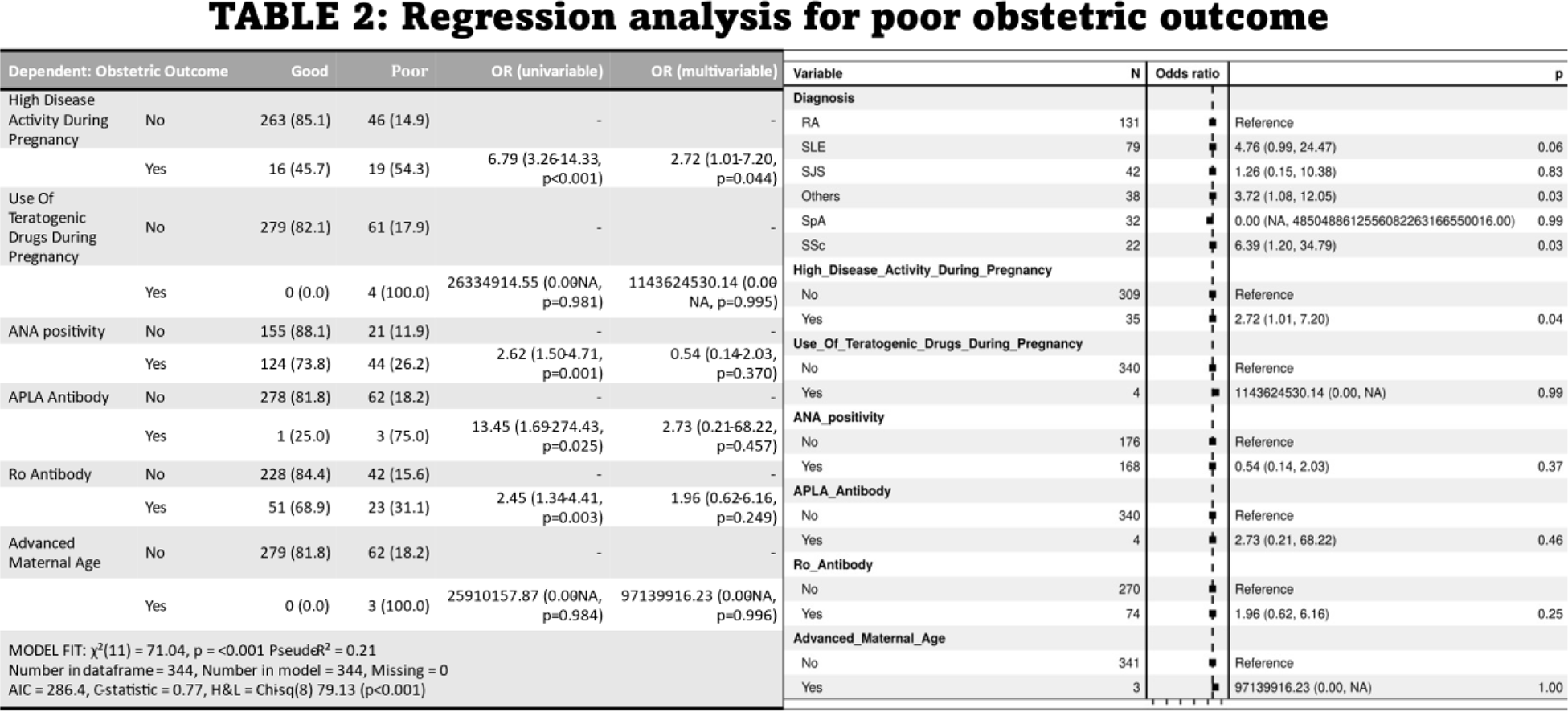
Results: The mean age for the study and control groups was 32.56 ± 6.98 years and 28.36 ± 4.76 years, respectively. (Table 1) presents a comparison of total pregnancy outcomes between the cases and the controls. The number of pregnancies was significantly higher in the cases (1.34 ± 1.20SD) compared to controls (0.74 ± 1.00SD). Four patients had advanced maternal age, while none in the control group did. Unplanned pregnancies were also more common in cases (0.56 ± 1.03SD) versus controls (0.04 ± 0.23SD). The rate of spontaneous abortions was higher in cases (0.25 ± 0.63SD) compared to controls (0.11 ± 0.31SD), but no significant differences in first and second-trimester abortions were noted. Regression analysis (Table 2) identified SLE as an independent risk factor for poor obstetric outcomes in univariate analysis, while high disease activity, ANA, APL, and Ro positivity did not influence the poor obstetric outcomes in this study, no significant differences were found in multivariate analysis.
Conclusion: This study demonstrates that pregnancy among women with AIRD, especially SLE with active severe organ involvement poses a significant risk of complications Patients planning to become pregnant must prioritize achieving remission or maintaining a stable state of low disease activity. It is essential that they optimize and maintain stable medication for at least six to twelve months before conception. Research clearly demonstrates that planned pregnancies in patients with systemic lupus erythematosus (SLE) result in significantly better outcomes compared to unplanned ones. This indicates the necessity of contraception at specific stages of the disease and during immunosuppressive therapy. Despite this understanding, counselling for women with SLE on contraception remains inadequate, as evidenced by a study published in Arthritis Care & Research. Once pregnant, women with SLE experience a notably higher risk of miscarriages and stillbirths. Approximately 20% of pregnancies in these women end in miscarriage, starkly contrasted with 9% in the general population. Our findings corroborate this alarming statistic within our SLE sample. Moreover, some studies reveal that this heightened risk can occur even before a diagnosis of SLE, with nearly a two-fold increase in miscarriage rates compared to controls. Miscarriages and stillbirths undoubtedly contribute to the reduced rate of live births. While previous research has asserted that pregnancy does not exacerbate rheumatoid arthritis (RA), pregnant mothers with RA are still at an increased risk of eclampsia, cesarean delivery, and preterm birth. It is important to counsel these patients about family planning and teratogenic medications. This is a descriptive, cross-sectional study conducted in a single center, which limits our capacity to draw causal conclusions. There was a discrepency in pregnancy outcomes among cases and control group because majority women in control group were unmarried and of a young age with lesser no of pregnancies. Further multicentric research is imperative to thoroughly investigate the impact of demographic, social, and clinical factors, allowing us to identify which subgroups of women are at the highest risk of poor obstetric outcomes.
REFERENCES: [1] Vinet, Evelyne et al. “Decreased live births in women with systemic lupus erythematosus.” Arthritis care & research vol. 63,7 (2011): 1068-72.
[2] Pina Vegas L, Drouin J, Weill A , et al. Pregnancy outcomes in women with rheumatoid arthritis: an 11-year French nationwide study. RMD Open 2024; 10: e003762.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (