fetching data ... 
Background: Systemic Lupus Erythematosus (SLE) is a chronic, systemic autoimmune disease associated with significant morbidity and mortality. These patients have a 3-4 times higher risk of mortality compared to the general population. Approximately 25% of SLE patients presenting to emergency departments require hospitalization, and 13-33% of these require intensive care unit (ICU) admission.
Objectives: To systematically review the literature evaluating the causes of hospitalization and ICU admission, clinical characteristics and mortality risk factors associated with SLE patients admitted to the ICU.
Methods: A systematic review of literature published between 2000 and 2024 was conducted using PubMed, EMBASE, Web of Science, and SCOPUS. The following Medical Subject Headings (MeSH) terms were used: “Systemic lupus erythematosus,” “autoimmune diseases,” “intensive care,” “critical care,” “intensive care unit,” “intensive care units,” “sepsis,” “septic shock,” and “Mortality.” Boolean operator “AND” was used to combine terms. English and Spanish articles were included, and reference lists of retrieved publications were manually searched. Cohort, case-control, and cross-sectional studies were included if they met the following criteria: (1) 20 or more adult SLE patients; (2) fulfillment of classification criteria (ACR 1997, SLICC-ACR 2012, or EULAR-ACR 2019); and (3) description of ICU admission causes, and outcomes.
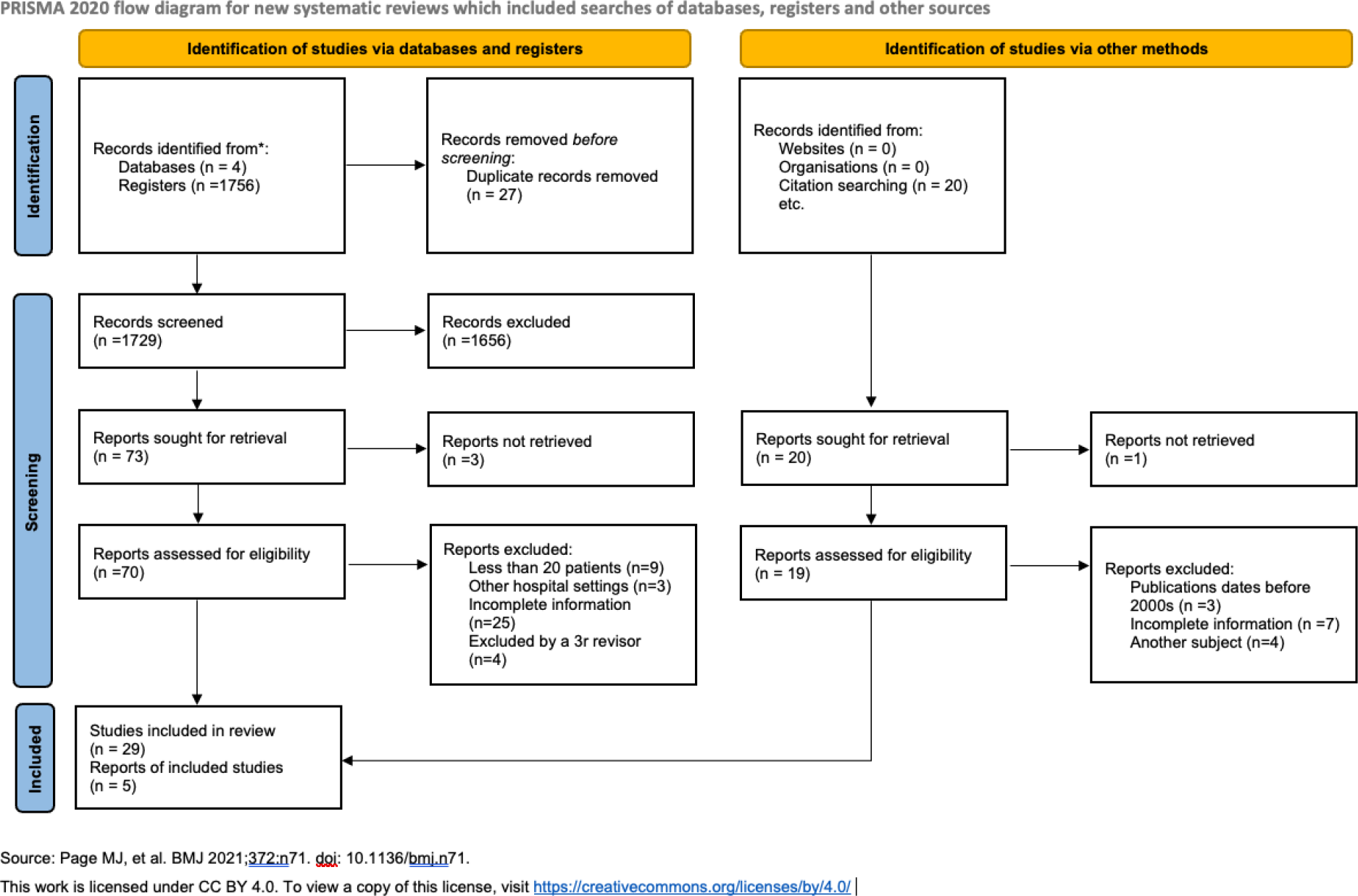
Results: A systematic review of 1756 studies identified 34 eligible studies that included 4769 SLE patients admitted ICUs (Figure 1). The average mortality rate was found to be 33.83%. Most patients were female (84.5%) with a mean age of 35.61 years. Common reasons for admission included infections (13-80.3%), respiratory failure (6.8-76.5%), shock (6.6-62.3%), lupus flare (14.2-55.6%), dialysis urgency (3.6-47.6%), and cardiovascular disease (3.2-44%). 27 studies (n=4456) evaluated predictors of mortality. Older age, lower socioeconomic status, and higher scores on severity indices like APACHE II (>19) and SLEDAI 2K (>12) were associated with increased mortality. Clinical factors such as infections, multiorgan failure, thrombocytopenia, and antiphospholipid syndrome also predicted poorer outcomes. Treatment-related factors, including the need for mechanical ventilation, vasopressors, and renal replacement therapy.
Conclusion: Our findings highlight the need for further research to develop targeted interventions for SLE patients in the ICU, particularly those aimed at preventing infections, improving organ support, and addressing socioeconomic disparities.
REFERENCES: NIL.
PRISMA 2020 flow diagram for new systematic reviews.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (