fetching data ... 
Background: Stress and other lifestyle components, including physical inactivity, obesity, poor diet, and disturbed sleep, contribute to systemic chronic low-grade inflammation which is a common driver of both rheumatoid arthritis (RA) and metabolic syndrome-associated osteoarthritis (MSOA) [1]. The Plants for Joints (PFJ) randomized controlled trials (RCT) investigated the effect of a multidisciplinary lifestyle intervention based on a whole food plant-based diet, physical activity, and sleep and stress management in people with low to moderately active RA or hip and/or knee MSOA [2]. After the 4-month intervention, disease activity was significantly decreased in people with RA (mean DAS28 –0.9 point), while those with MSOA had significantly less pain and stiffness and improved physical function (mean Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score –11 points). Given the effect of stress-management interventions on inflammation and disease outcomes in previous studies, it is hypothesised that the stress-component of the PFJ intervention contributed to its clinical effectiveness.
Objectives: This secondary analysis aimed to evaluate the effect of the PFJ intervention on stress-related parameters.
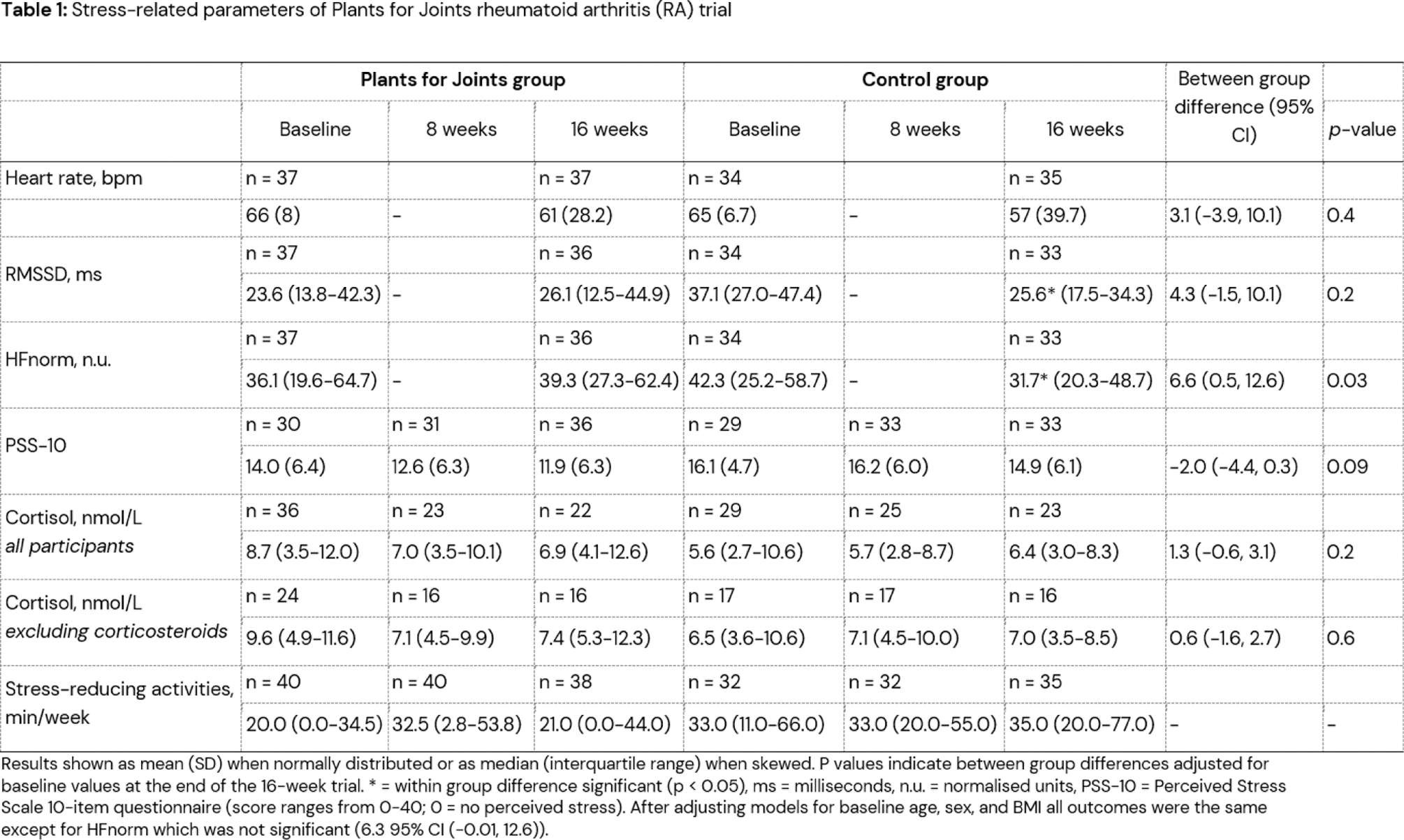
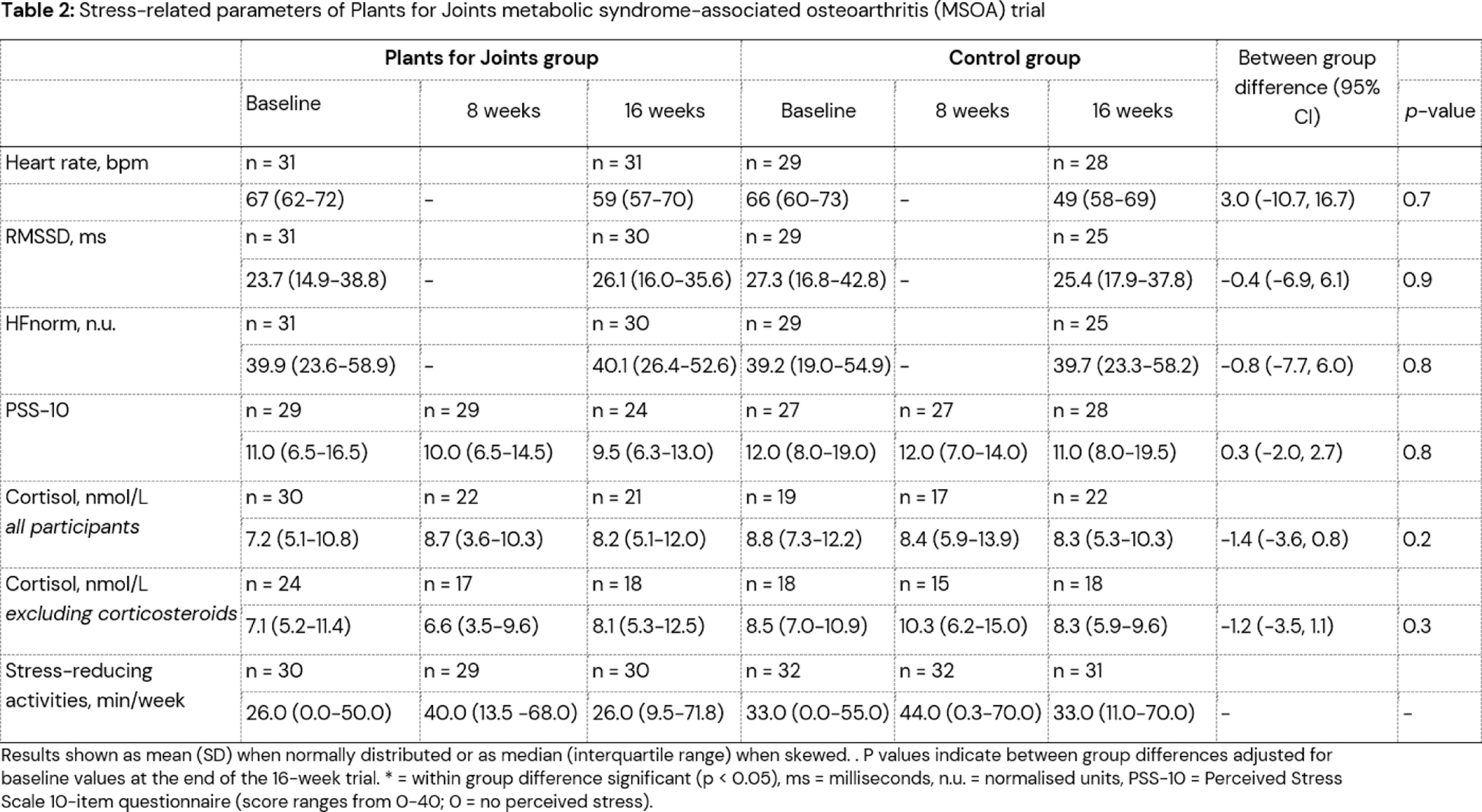
Methods: In two PFJ observer-blind RCTs, people with (1) RA or (2) MSOA were randomized to receive the PFJ lifestyle intervention or usual care. The 16-week PFJ intervention consisted of a whole-food plant-based diet, physical activity, and sleep and stress management. This secondary analysis investigated stress-related outcomes including heart rate, heart rate variability (HRV: root square mean of successive differences (RMSSD) and normalized high frequency (HFnorm), salivary cortisol, perceived stress (Perceived Stress Scale 10; PSS-10), and time spent on stress-reducing activities. An intention-to-treat analysis with a linear regression model (heart rate and HRV) or linear mixed model (cortisol and PSS-10), adjusted for baseline values, was used to analyse between-group differences. Associations between stress-reducing activities and stress-related parameters were assesed using Pearson’s (normally distributed data) or Spearman’s (skewed data) correlation coefficients.
Results: 77 people with RA and 64 with MSOA completed the RCTs. RA participants following the PFJ intervention showed a significant improvement in HFnorm (between-group difference: 6.6; 95% CI 0.5, 12.6) and an improving trend in RMSSD (4.3; 95% CI -1.5, 10.1) alongside non-significant reductions of heart rate (3.1; 95% CI-3.9, 10.1), salivary cortisol (1.3; 95% CI -0.6, 3.1) and perceived stress (–2.0; 95% CI -4.4, 0.3), compared to usual care. In participants with MSOA, there were no differences in heart rate, HRV outcomes, cortisol, or perceived stress between the intervention and control group. Both RA and MSOA participants temporarily increased time spent on stress-reducing activities, yet no change from baseline was observed after 16 weeks and no significant correlations between the different stress-related parameters and the number of stress-reducing activities was found.
Conclusion: This secondary analysis of two randomized controlled trials on the effects of the Plants for Joints (PFJ) lifestyle intervention suggests a potential positive impact on stress-related parameters in people with RA, but not MSOA, compared to usual care. While participants only showed short-term increase observed time spent on stress-reducing activities, the intervention as a whole, other lifestyle components, or unquantified stress-related changes such as improved disease activity may have contributed to reduced stress levels. These stress-related improvements may contribute to the observed clinical effectiveness of the PFJ intervention in people with RA.
REFERENCES: [1] Furman, D., et al., Chronic inflammation in the etiology of disease across the life span. Nat Med, 2019. 25 (12): p. 1822-1832.
[2] Walrabenstein, W., et al., A multidisciplinary lifestyle program for rheumatoid arthritis: the ‘Plants for Joints’ randomized controlled trial. Rheumatology (Oxford), 2023. 62 (8): p. 2683-2691.
Acknowledgements: Study participants of the “Plants for Joints” trial, patient partners of “Plants for Joints”, employees of the Reade Biobank (Toni de Jong-de Boer and Corrie Verdoold), registered dietitians Pauline Kortbeek, Anna Kretova, Melissa Dijkshoorn, Marieke van de Put and Dana Hofland, exercise coaches Sietske de Weers, Tom van Iersel and Jobjan Blonk, physical therapist Boke Dekker and relaxation/sleep coaches Nelleke Doornebal and Marieke Rinkema. We thank the Endocrinology lab from the Amsterdam UMC, for technical support.
Disclosure of Interests: Jeroen Christiaans: None declared, Carlijn Wagenaar Honoraria for lectures from Abbvie and from i’m a Foodie, Author holds shares in Plants for Health, a limited liability company, which aims to have a positive impact on society and the environment and provide an adapted version of the Plants for Joints program as an additional treatment option for people with rheumatic conditions, Veerle Hermans: None declared, Wendy Walrabenstein Author holds shares in Plants for Health, a limited liability company, which aims to have a positive impact on society and the environment and provide an adapted version of the Plants for Joints program as an additional treatment option for people with rheumatic conditions, Frieda Koopman: None declared, Henriët van Middendorp: None declared, D. van Schaardenburg Author holds shares in Plants for Health, a limited liability company, which aims to have a positive impact on society and the environment and provide an adapted version of the Plants for Joints program as an additional treatment option for people with rheumatic conditions.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (