fetching data ... 
Background: Interstitial lung disease (ILD) is a major complication in systemic sclerosis (SSc) patients as it is associated with increased mortality and significant morbidity. Rituximab (RTX) and mycophenolate mofetil (MMF) are both recommended treatments for SSc-ILD, according to the recent update in EULAR recommendations [1]. Combination therapies are foreseen as the future of SSc-ILD management and a recent trial suggested that the combination of RTX and MMF might be superior to MMF alone in connective tissue disease (CTD) patients with ILD [2].
Objectives: To compare outcomes at 12 months in patients with SSc-ILD treated with RTX alone, MMF alone, or upfront combination therapy (MMF + RTX).
Methods: SSc patients meeting the 2013 ACR/EULAR criteria, with ILD confirmed by chest HRCT and available % predicted FVC (%pFVC) at baseline and 12 ± 3 months, were eligible for inclusion. Patients were grouped based on treatment initiated at baseline: (a) MMF alone, (b) RTX alone, or (c) upfront combination therapy (MMF + RTX). Patients on nintedanib or tocilizumab at baseline were excluded. Inverse probability of treatment weighting (IPTW) was used to adjust for confounding and treatment imbalances, following multiple imputation for missing data. Propensity score models incorporated the following variables: age, gender, disease subset (diffuse vs. limited), autoantibody status (ATA positivity), baseline FVC, and disease duration. Linear mixed-effects models were used to compare the change in %pFVC and DLCO% at 12 ± 3 months across groups. The proportion of patients with ILD progression (FVC decline >5%) was also calculated.
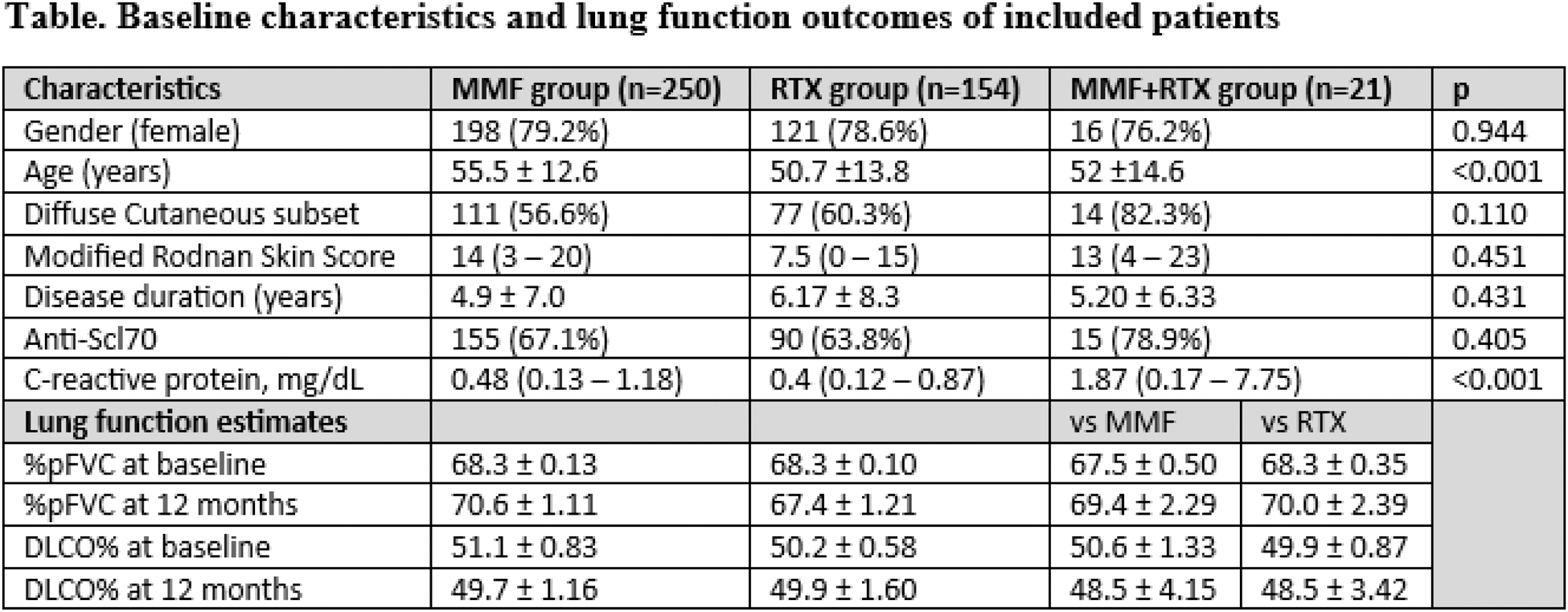
Results: A total of 425 patients were included in the final analysis (250 MMF, 154 RTX and 21 combination therapy). Baselines characteristics and outcomes are summarized in the Table 1. At 12 months, FVC remained stable in all treatment groups. In model 1 (MMF vs. combination), the mean change in FVC was 2.28% (95%CI 0.10 — 4.40) for MMF vs 1.83% (95%CI -2.8 — 6.5) for the combination group (mean difference -0.44, 95%CI -5.70 — 4.80, p = 0.867). The mean change in DLCO was -1.35% (95%CI -3.92 — 1.21) for MMF vs -2.05% (95%CI -11.2 — 7.14) for the combination group (mean difference -0.7, 95%CI -10.0 — 8.61, p = 0.882). In model 2 (RTX vs. combination), the mean change in FVC was -0.93% (95%CI -3.29 — 1.43) for RTX vs 1.71% (95%CI -2.97 — 6.41) for the combination group (mean difference 2.65, 95%CI -2.52 — 7.82, p = 0.315). The mean change in DLCO was -0.35% (95%CI -3.48 — 2.78) for RTX vs -1.43% (95%CI -8.6 — 5.73) for the combination group (mean difference -1.08, 95%CI -8.71 — 6.54, p = 0.781). The proportion of patients with ILD progression at 12 months was similar across treatment groups: MMF 29.2% (95%CI 23.3-35.1), RTX 28.1% (95%CI 20.2-36.0), and combination therapy 27.4% (95%CI 5.9-48.8).
Conclusion: This EUSTAR cohort analysis does not demonstrate a clear benefit of upfront combination therapy with MMF and RTX over treatment with either agent alone regarding FVC decline at 12 months in SSc-ILD patients. Further studies are required to better understand the role of combination therapy specifically for SSc-ILD.
REFERENCES: [1] Del Galdo F, et al. EULAR recommendations for the treatment of systemic sclerosis: 2023 update. Ann Rheum Dis. 2024 Oct 17:ard-2024-226430.
[2] Mankikian J et al. Rituximab and mycophenolate mofetil combination in patients with interstitial lung disease (EVER-ILD): a double-blind, randomised, placebo-controlled trial. Eur Respir J. 2023 Jun 8;61(6):2202071.
Table 1.
Acknowledgements: We are grateful to all the EUSTAR centers who participated in this study.
Disclosure of Interests: Devis Benfaremo: None declared, Corrado Campochiaro: None declared, Gábor Kumánovics: None declared, Christina Bergmann Kyverna therapeutics, Elisabetta Zanatta: None declared, David Launay: None declared, Serena Guiducci: None declared, Mickael Martin: None declared, CAROLINA SOUZA MULLER: None declared, Carlomaurizio Montecucco: None declared, Luc Mouthon: None declared, Gabriella Szucs: None declared, Kastriot Kastrati: None declared, Marie-Elise Truchetet: None declared, Madelon Vonk Janssen Pharmaceutical Companies of Johnson & Johnson, MSD, Novartis, and Roche, Boehringer Ingelheim and Janssen Pharmaceutical Companies of Johnson & Johnson, Francesco Del Galdo Abbvie, Argenx, AstraZeneca, Boehringer-Ingelheim, Capella, Calluna, Chemomab, DeepCure, Ergomed,GSK, Janssen, Mitsubishi-Tanabe, MSD, Novartis, Serono,Ventus, Abbvie, Argenx, AstraZeneca, Boehringer-Ingelheim, Capella, Calluna, Chemomab, DeepCure, Ergomed,GSK, Janssen, Mitsubishi-Tanabe, MSD, Novartis, Serono,Ventus, Marco Matucci-Cerinic: None declared, Gianluca Moroncini: None declared, Yannick Allanore: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (