fetching data ... 
Background: The COMPLETE PsA trial was a single center, investigator initiated, double-blind, randomized, placebo-controlled trial. This trial showed that a combination therapy with methotrexate (MTX) and leflunomide (LEF) is superior compared to MTX monotherapy regarding efficacy after 4 months in patients with PsA [1]. However, the combination is also associated with higher risk of adverse events. The latest EULAR recommendations on pharmacological management of PsA do not recommend using the combination due to the low efficacy to safety ratio [2]. It is not known yet whether the strategy of starting with combination translates to better outcomes in the long-term. Currently, long-term follow-up data in standard care of patients who participated in the COMPLETE PsA trial are available, enabling a long-term analysis, especially focused on drug survival, and time to first biological Disease Modifying Anti-Rheumatic Drug (bDMARD).
Objectives: The aims of this study are to 1/ compare the long-term drug survival (tolerability) of the strategy of initial MTX and LEF combination therapy to initial MTX monotherapy in psoriatic arthritis and 2/ assess differences in time to first bDMARD (efficacy).
Methods: All consenting patients who completed the COMPLETE PsA trial, were included in this long term extension cohort study, with start of the original COMPLETE PsA trial as baseline. Patients were censored after 24 months of follow-up. Data on patient- and disease characteristics and medication use were obtained from the Integrated rheumatology information system (IRIS) and electronic health records of the Sint Maartenskliniek. To asses tolerability, the drug survival of MTX and LEF combination therapy and MTX monotherapy were analysed and compared and reasons for discontinuation were assessed. Discontinuation of either MTX or LEF in the combination therapy group and MTX in the monotherapy group was counted as an event. Pregnancy or remission as reason for discontinuation were censored. In addition, to assess efficacy, the time to start the first bDMARD was analysed and compared between the two originally allocated groups. All analyses were performed using the Kaplan-Meier (KM) method and univariate significance of the time to event tested using the log-rank test.
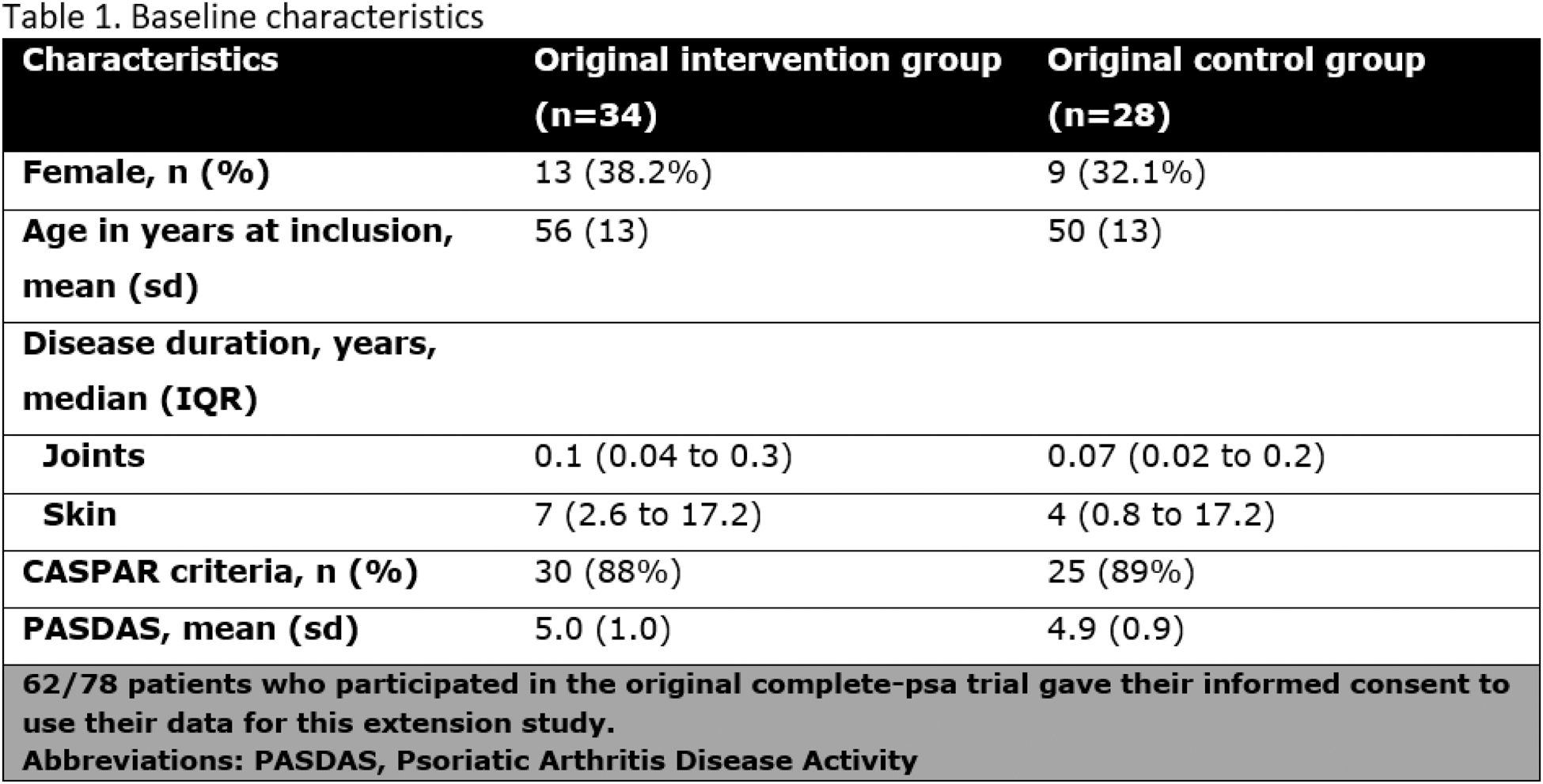
Results: 62/78 patients consented and were included (34 intervention group and 28 control group patients). Baseline characteristics were similar between groups (Table 1). Median follow-up was 50 months (43 to 61) in the MTX + LEF group and 46 months (42 to 57) in the MTX group. Loss to follow-up at 24 months did not differ between groups 8.8% and 11% respectively. The KM estimated drug survival of MTX and LEF combination therapy at 6, 12 and 24 months follow-up was 44% (95%CI: 27% to 60%), 35% (95%CI: 19% to 51%) and 27% (95%CI: 13% to 43%), respectively. For MTX monotherapy this was 60% (95%CI: 40% to 76%), 46% (95%CI: 28% to 63%) and 33% (95%CI: 16% to 51%), respectively (log rank test p=0.24,(Figure 1A)). Reasons for discontinuation were inefficacy (26%) and tolerability (74%). 53% (18/34) patients in the original intervention group and 54% (15/28) patients in the original control group started a bDMARD during the follow-up period, with KM estimated cumulative incidence at 6, 12 and 24 months follow-up of 29%, 44% and 64% in the original intervention group and 4.2%, 37% and 54% in the control group, respectively (log rank test p=0.38) (Figure 1B).
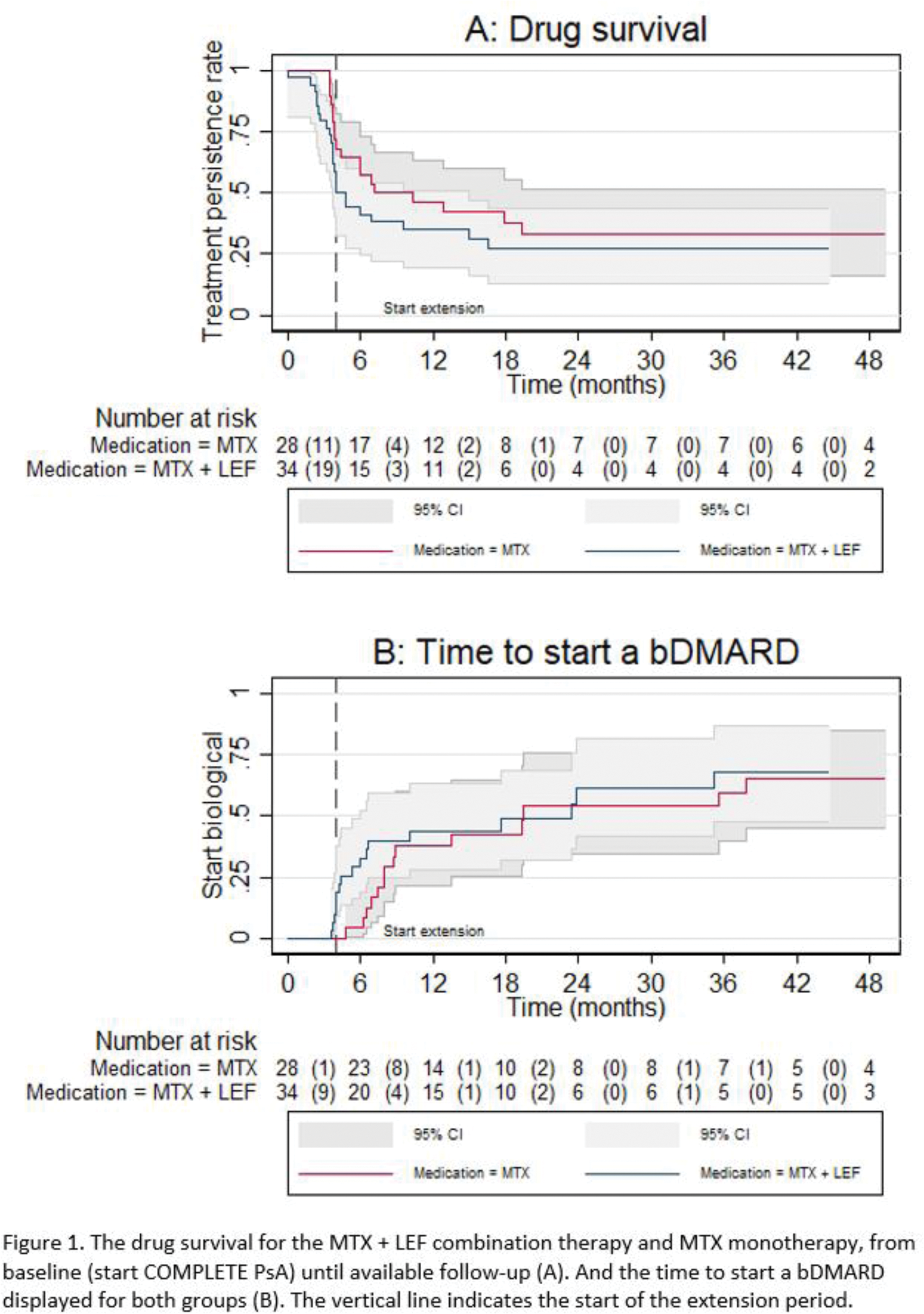
Conclusion: While the COMPLETE-PsA showed superior efficacy of MTX + LEF over MTX alone on the short term, this extension study shows (1) the drug survival of csDMARDs rapidly declined in both groups and (2) the subsequent time to start a bDMARD initiation was not delayed in the combination group. This might, be due to lower tolerability of the combination therapy.
REFERENCES: [1] Comparing methotrexate monotherapy with methotrexate plus leflunomide combination therapy in psoriatic arthritis (COMPLETE-PsA): a double-blind, placebo-controlled, randomised, trial. Mulder, Michelle L M et al. The Lancet Rheumatology, Volume 4, Issue 4, e252 - e261.
[2] Gossec L, Kerschbaumer A, Ferreira RJO , et al EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2023 update Annals of the Rheumatic Diseases 2024;83:706-719.
Acknowledgements: NIL.
Disclosure of Interests: Amy C D Peeters: None declared, Nathan den Broeder: None declared, Michelle L M Mulder Yes, speaker fee from Novartis, Yes, consultant fee from Novartis, Laura C. Coates Laura Coates has been paid as a speaker for AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer and UCB, Laura Coates has worked as a paid consultant for AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Enlivex, Janssen, Moonlake, Novartis, Pfizer, Takeda and UCB, Laura Coates has received grants/research support from Abbvie, Amgen, Janssen and UCB, Emmerik F.A. Leijten Received grants from Novartis and Eli Lilly, made out to the institution, for research and quality of care projects (unrelated to the work in the manuscript), Johanna E. Vriezekolk -, A.A. den Broeder Alfons den Broeder received research and quality of care grants to the institution Sint Maartenskliniek from Abbvie, Lilly, UCB, Celltrion, Biogen, Sanofi, Gilead, Galapagos, Alfasigma, Novartis, Pfizer, Johnson&Johnson, Noortje van Herwaarden Noortje van Herwaarden received speakers fee from Pfizer and Alfasigma, Noortje van Herwaarden received research and quality of care grants to the institution Sint Maartenskliniek from Celltrion, Lilly and Novartis.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (