fetching data ... 
Background: Psoriatic Arthritis (PsA) is a heterogeneous disease that necessitates multidisciplinary care due to its diverse manifestations and associated comorbidities, posing unique challenges in both diagnosis and management. Despite advances in therapeutic options, a significant subset of patients remains unable to achieve or maintain sustained remission. Definitions of treatment failure in Psoriatic Arthritis (PsA) are lacking, in contrast to the published criteria for rheumatoid arthritis [1] and the recently outlined criteria for axial spondyloarthritis [2]. To address this gap, the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) initiated a research project aimed at developing definitions of D2T and C2M PsA, which could be a starting point to disentangling the myriad of treatment inefficacies in PsA.
Objectives: The GRAPPA research project aims to establish robust, consensus-driven definitions for Difficult-to-Treat (D2T-) PsA, characterized by persistent inflammation despite the use of multiple advanced therapies, and Complex-To-Manage (C2M-) PsA, which includes D2T plus broader factors such as comorbidities, chronic non-inflammatory pain, or treatment intolerance. This initiative seeks to facilitate future targeted research and tailored clinical approaches.
Methods: The project leveraged a comprehensive approach, beginning with a scoping literature review and global surveys conducted among GRAPPA healthcare professionals (n=223) and PsA patients (n=570) to capture diverse experiences and perspectives. Insights from these surveys guided a multidisciplinary working group, consisting of rheumatologists, dermatologists, patient research partners, and Young-GRAPPA representatives from diverse regions, in formulating initial definitions. These definitions were further refined through comprehensive discussions and considering the wider GRAPPA membership’s voice. This process was followed by a structured two-round Delphi exercise within the working group to achieve consensus (≥70% agreement). The proposed definitions and overarching principles were ultimately brought to the GRAPPA membership for endorsement via an online voting.
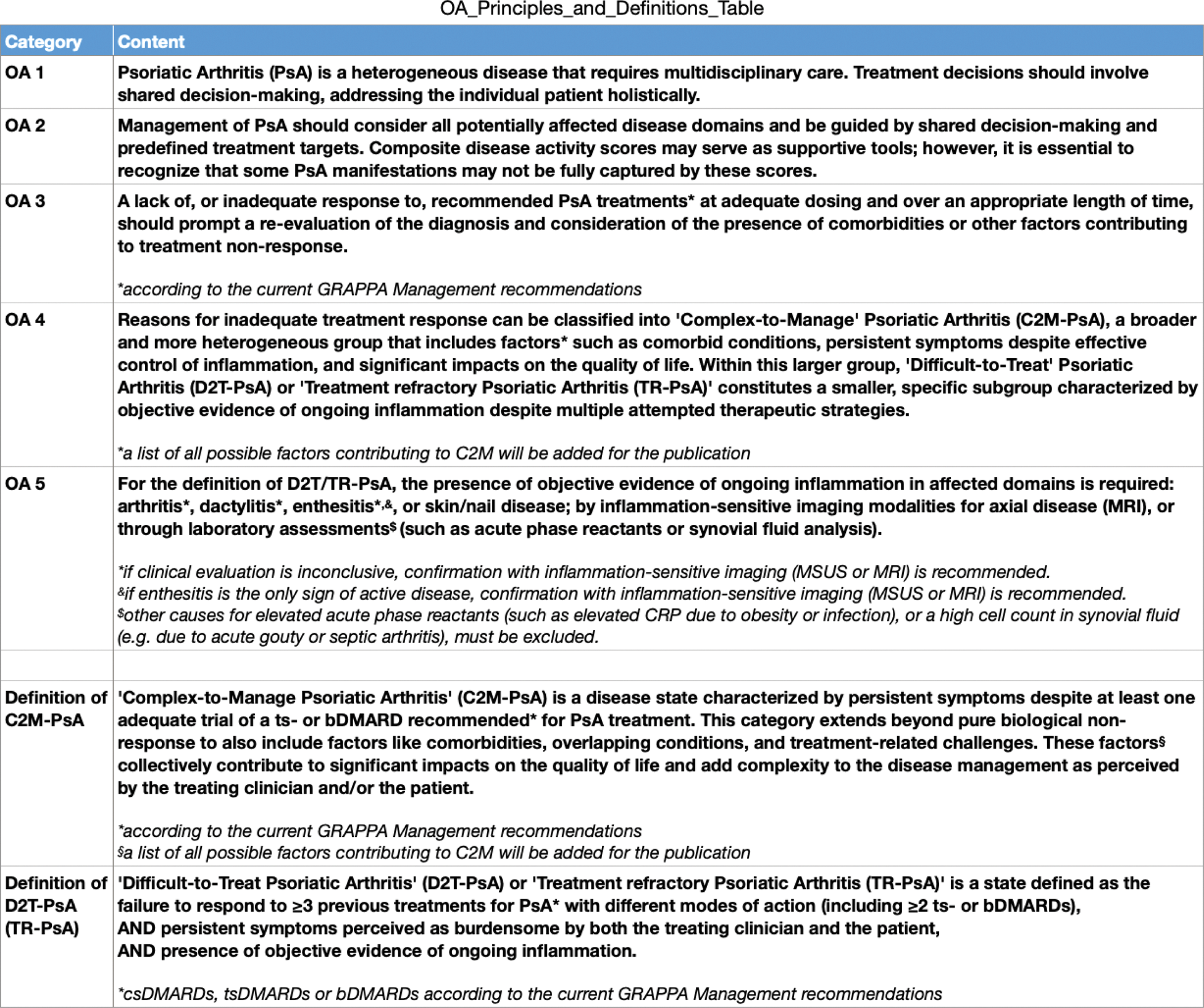
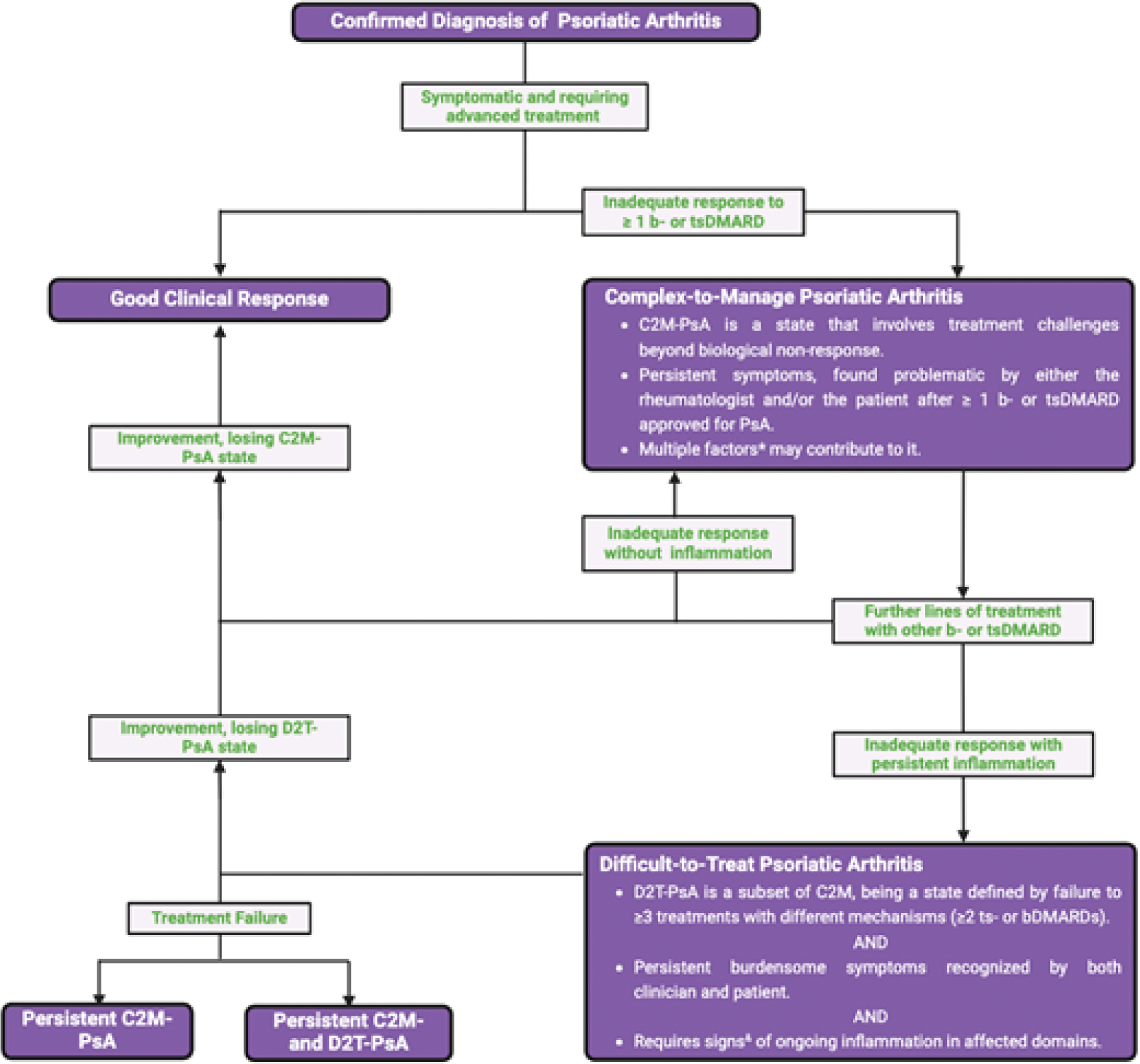
Results: The initiative led to the development of five overarching principles and the introduction of novel definitions for D2T-PsA and C2M-PsA (Table 1). ‘Difficult-to-Treat PsA’, also referred to as ‘Treatment-Refractory PsA’ (TR-PsA), represents a distinct subset within Complex-To-Manage PsA, characterized by objective evidence of persistent inflammation despite multiple therapeutic strategies (≥3 previous treatments for PsA with different modes of action (including ≥2 ts- or bDMARDs). This classification is particularly valuable for research and clinical trials, enabling the identification of homogeneous patient populations for targeted interventions. In contrast, C2M-PsA encompasses a broader scope, incorporating other factors that complicate disease management, such as comorbidities, chronic pain, treatment intolerance, and psychosocial challenges. This definition is designed for broader clinical application, addressing diverse aspects of patient care, including quality of life and overall impact of the disease (Figure 1). The overarching principles and definitions (Table 1) have received strong endorsement from the GRAPPA membership, with 95.1% (175 out of 184 responses) voting in favor.
Conclusion: The GRAPPA initiative has established consensus definitions for D2T- and C2M-PsA, addressing critical gaps in PsA care. These definitions provide a framework for recognizing patients with persistent inflammation unresponsive to advanced therapies (D2T-PsA) and those facing broader management challenges, including comorbidities and psychosocial factors (C2M-PsA). By improving patient stratification, guiding clinical decision-making, and standardizing criteria for clinical trials, this work provides the foundation for advancing both research and clinical care, and potentially improve outcomes for patients with the most complex and refractory disease presentations in the future.
REFERENCES: [1] Nagy G. et al.; EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. 2021 Jan;80(1):31-35.
[2] Poddubnyy D. et al.; The Assessment of SpondyloArthritis International Society (ASAS) Definition of Difficult-to-Manage Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9).
Table 1. Overarching principles and definitions for C2M- and D2T-PsA.
Algorithm of treatment failure in PsA with Complex-To-Manage PsA and Difficult-To-Treat PsA.
Acknowledgements: We extend our deepest gratitude to all the patients who participated in this study, lending invaluable insights and experiences. We are thankful for the collaborative support from our colleagues and contributors, including Nicolas Chronis, Cameron Hay-Rollins, Murat Torgutalp, and the translators who facilitated communication across languages. Our appreciation also goes to the entire GRAPPA membership, the GRAPPA Research Committee, and the GRAPPA Administration for their continuous support and commitment to this project. A special tribute is owed to Deepak Jadon, whose foundational contributions were vital to our endeavors until his untimely departure. His legacy continues to inspire and drive our work forward.
Disclosure of Interests: Fabian Proft Speakers bureau with payments made directly to me for: AbbVie, AMGEN, BMS, Celgene, Eli Lilly, Hexal, Janssen, Medscape, MSD, Novartis, Pfizer, Roche and UCB, Consultancy with payments made directly to me for: AbbVie, BMS, Janssen, Novartis, Pfizer and UCB, Grant/research support from Novartis, Eli Lilly and UCB with payments made via my institution, Andre Lucas Ribeiro Speaker’s bureau: AbbVie, Johnson & Johnson, Shikha Singla Speaker’s bureau: Janssen, Consultant: AbbVie, Janssen, UCB; Research grants: Eli Lilly, Prometheus Biosciences, Vinod Chandran Spousal employment: AstraZeneca, Consulting/Advisory boards: AbbVie, BMS, Eli Lilly, Fresenius Kabi, Johnson and Johnson, Novartis, and UCB, Research grants: Eli Lilly and Johnson and Johnson, Wilson Liao Research grants: Amgen, Janssen, Leo, Regeneron, Christine Lindsay Stocks: Amgen, Arcutis, Enrique R. Soriano Speaker’s bureau: AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer, Roche, and UCB, Consultant: AbbVie, Janssen, Novartis, and Roche, Grant/research support: AbbVie, Janssen, Novartis, Pfizer, Roche, and UCB, Tina Bhutani Speaker for Amgen, Arcutis, Galderma, Janssen, Lilly and Leo, Advisor for Abbvie, Arcutis, Aslan, Boehringer-Ingelheim, Bristol Myers Squibb, Dermavant, Galderma, Incyte, Janssen, Leo, Lilly, Pfizer, Novartis, Sanofi, Sun, Takeda, and UCB, Research funding from Amgen, Castle, CorEvitas, Novartis, Pfizer, and Regeneron, Atul Deodhar Consultant: BMS, Eli Lilly, J&J, MoonLake, Novartis, Pfizer and UCB, Grant/research support: BMS, Eli Lilly, J&J, MoonLake, Novartis, Pfizer, and UCB, Kurt de Vlam Consultant: BMS, Eli Lilly, J&J, MoonLake, Novartis, Pfizer and UCB, Grant/research support: Eli Lilly,Amgen, AlphaSigma and UCB, Lihi Eder Consultation/Ad board: Abbvie, BMS, Moonlake, J&J, Pfizer, Eli Liily, Novartis, UCB, Grants: Abbvie, J&J, Pfizer, Eli Liily, Novartis, UCB, Fresenius Kabi, Mitsumasa Kishimoto Consultant and/or Speaker’s bureau: AbbVie, Amgen, Asahi Kasei Pharma, Ayumi Pharma, Bristol Myers Squibb, Chugai, Daiichi Sankyo, Eisai, Eli Lilly, Gilead, Janssen, Novartis, Tanabe-Mitsubishi, and UCB Pharma, Ying-Ying LEUNG Speaker’s bureau: AbbVie, DKSH, Janssen, Novartis, and Pfizer, Ennio Lubrano: None declared, Dennis McGonagle Abbvie, BMS, Celgene, J&J, Lilly, Moonlake, Novartis, Pfizer, UCB, Denis Poddubnyy Speaker fees from AbbVie, Canon, DKSH, Eli Lilly, Janssen, MSD, Medscape, Novartis, Peervoice, Pfizer, and UCB, Consulting fees from AbbVie, Biocad, Bristol-Myers Squibb, Eli Lilly, Janssen, Moonlake, Novartis, Pfizer, and UCB, Research support from AbbVie, Eli Lilly, Janssen, Novartis, Pfizer and UCB, Laura Savage: None declared, Filip van den Bosch Consultant and/or Speaker’s bureau: Abbvie, Alfasigma, Eli Lilly, Fresenius Kabi, Grey Wolf Therapeutics, Janssen, Novartis and UCB, Consultant and/or Speaker’s bureau: Abbvie, Alfasigma, Eli Lilly, Fresenius Kabi, Grey Wolf Therapeutics, Janssen, Novartis and UCB, Philip J. Mease AbbVie, Amgen, Eli Lilly, Johnson & Johnson, Novartis, Pfizer, UCB, AbbVie, Acelyrin, Amgen, Bristol Meyers Squib, Century, Cullinan Biotech, Eli Lilly, Inmagene, Johnson & Johnson, Moonlake, Novartis, Pfizer, Takeda, UCB, AbbVie, Acelyrin, Amgen, Bristol Meyers Squib, Eli Lilly, Johnson & Johnson, Novartis, Pfizer, UCB,
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (