fetching data ... 
Background: Uric acid transporter 1 (URAT1) is responsible for the reabsorption of approximately 90% of uric acid (UA) in the kidneys [1]. Inhibitors targeting URAT1 can effectively increase the excretion of uric acid, thereby reducing serum UA (sUA) levels. Ruzinurad is a highly selective and potent inhibitor against URAT1. In previous phase 1 and phase 2 studies, ruzinurad was well-tolerated and showed robust sUA lowering effect in patients with hyperuricemia [2].
Objectives: We further conducted a phase 3 study to assess the efficacy and safety of ruzinurad versus allopurinol in patients with hyperuricemia associated with primary gout (NCT04956432).
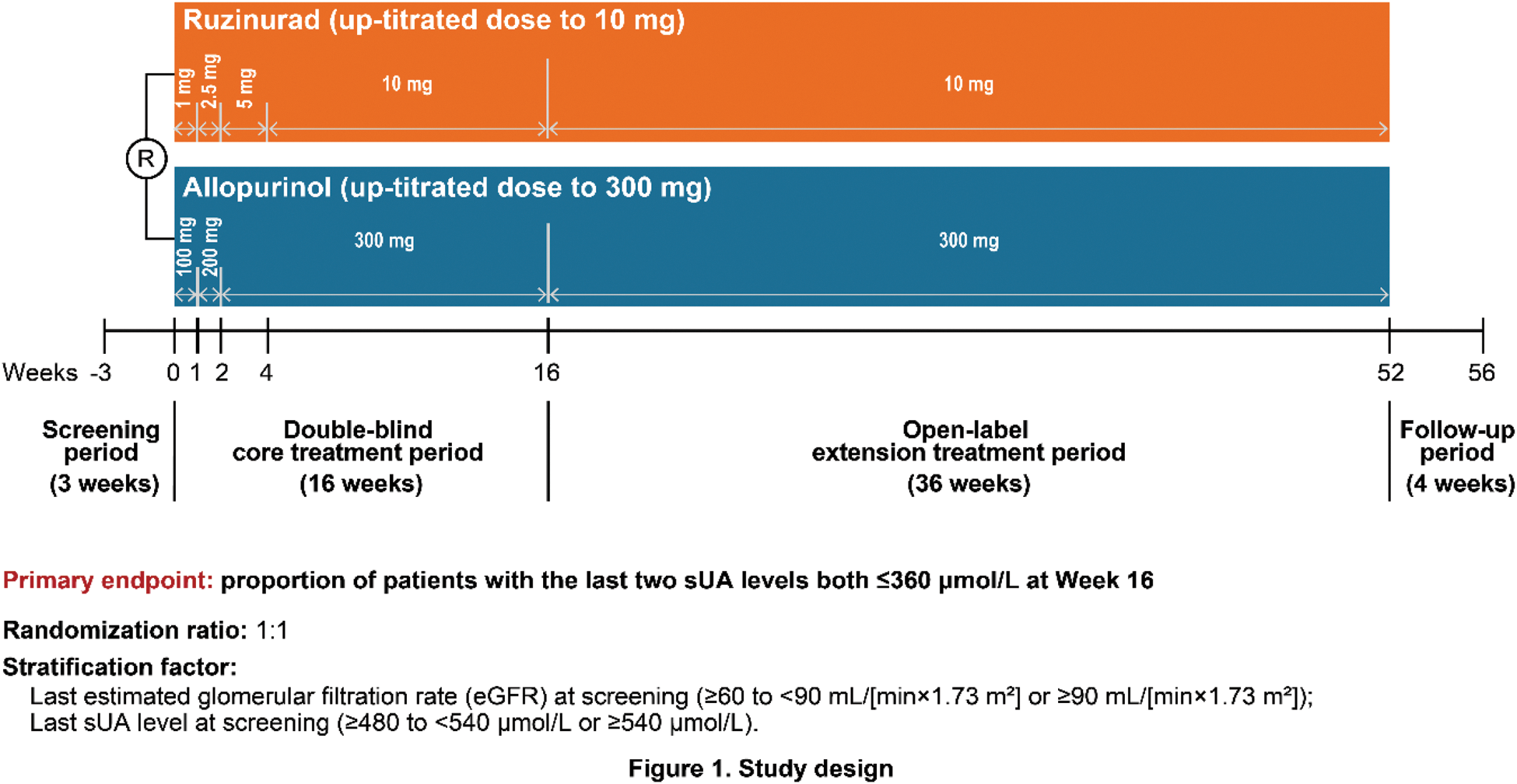
Methods: This was a multicenter, randomized, double-blind, active-controlled, phase 3 study consisting of a 3-week screening period, a 16-week double-blind core treatment period, a 36-week open-label extension treatment period, and a 4-week follow-up period (Figure 1). Gout adults with fasting sUA ≥480 µmol/L were randomly assigned (1:1) to the ruzinurad or allopurinol groups, stratified by the last estimated glomerular filtration rate (eGFR) at screening (≥60 to <90 mL/[min×1.73 m 2 ] or ≥90 mL/[min×1.73 m 2 ]) and the last sUA level at screening (≥480 to <540 μmol/L or ≥540 μmol/L). Treatment administration in the ruzinurad and allopurinol groups was initiated at 1 mg/day and 100 mg/day, followed by dose titration to 10 mg/day and 300 mg/day, respectively (Figure 1). All study medications were taken orally once daily. The primary endpoint was proportion of patients with the last two sUA levels both ≤360 μmol/L at Week 16.
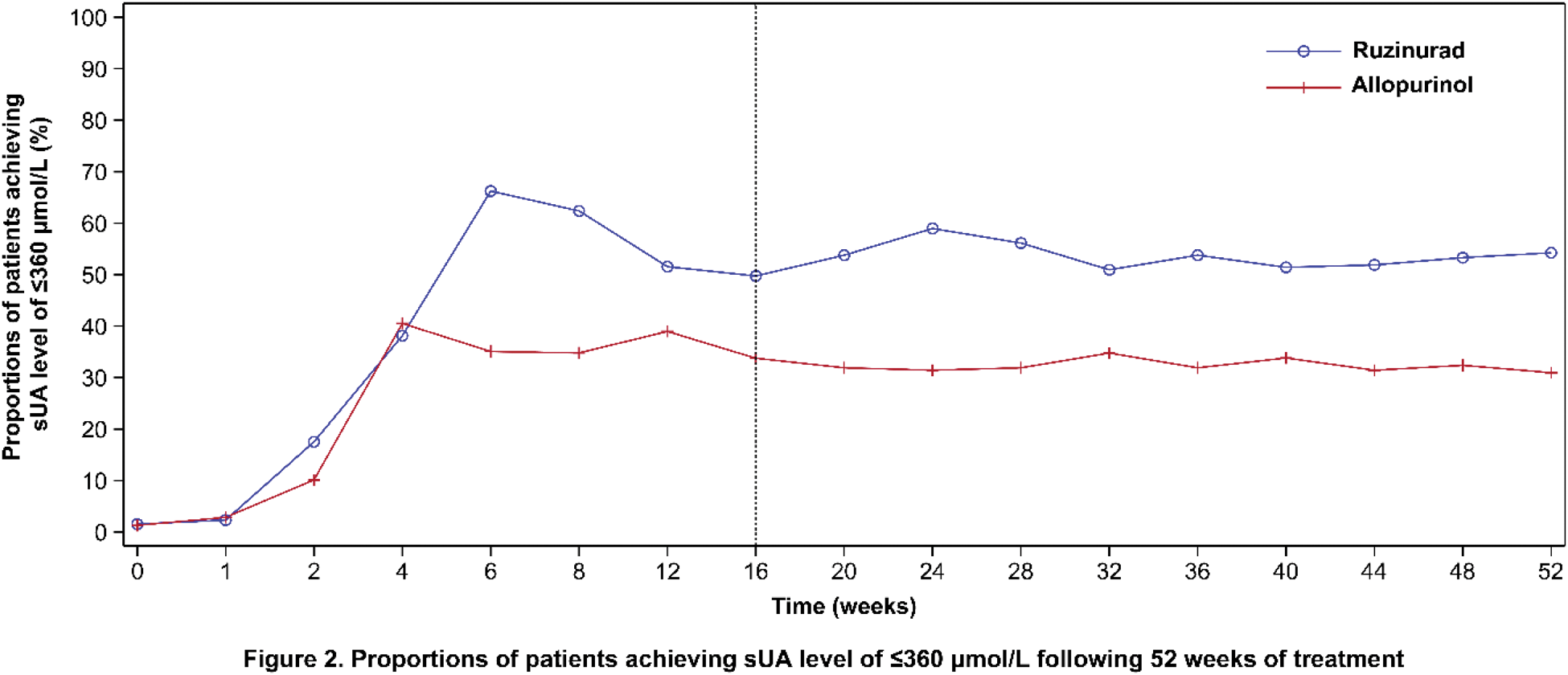
Results: A total of 773 patients received study treatment during the core treatment period, with 388 in the ruzinurad group and 385 in the allopurinol group. Baseline characteristics were generally balanced among the ruzinurad and allopurinol groups (male, 98.7% vs. 98.7%; median age, 35.0 vs. 36.0 years; median sUA, 576.5 vs. 568.0 μmol/L; eGFR <90 mL/(min×1.73 m 2 ), 34.8% vs. 35.3%; median creatinine, 83.0 vs. 82.0 μmol/L; absence of tophi, 85.3% vs . 87.0%; prior use of urate-lowering medications, 64.4% vs. 67.0%). At Week 16, significantly greater proportions of patients in the ruzinurad group achieved the target sUA level of ≤360 μmol/L at the last two monthly measurements, compared with the allopurinol group (39.7% [95% CI, 34.8% to 44.8%] vs. 26.5% [95% CI, 22.2% to 31.2%]; treatment difference, 13.1% [95% CI, 6.6% to 19.7%]; one-sided p <0.0001). Proportion of patients achieving sUA level of ≤360 μmol/L at Week 16 was greater in the ruzinurad group (52.6% vs. 34.5%; one-sided nominal p <0.0001), which was maintained until Week 52 (the end of extension treatment period; 54.2% in the ruzinurad group vs. 31.0% in the allopurinol group; Figure 2). During the 52-week treatment period, treatment-emergent adverse events (TEAEs) occurred in 348 (89.7%) and 353 (91.7%) patients in the ruzinurad and allopurinol groups, respectively, with the most common (≥20%) being gout flares (51.0% vs. 43.6%), increased alanine aminotransferase (21.6% vs. 29.4%), upper respiratory tract infection (21.4% vs. 19.0%), and increased blood creatinine (20.1% vs. 9.6%). The majority of TEAEs were mild or moderate. Serious TEAEs occurred in 4.9% and 3.1% of patients in the ruzinurad and allopurinol groups, respectively.
Conclusion: The URAT1 inhibitor ruzinurad demonstrated superior sUA lowering effect over allopurinol, along with a well-tolerated safety profile, in patients with hyperuricemia associated with primary gout.
REFERENCES: [1] So A, Thorens B. Uric acid transport and disease. J Clin Invest. Jun 2010;120(6):1791-9. doi:10.1172/jci42344
[2] Lin Y, Chen X, Ding H, et al. Efficacy and safety of a selective URAT1 inhibitor SHR4640 in Chinese subjects with hyperuricaemia: a randomized controlled phase II study. Rheumatology. 2021;60(11):5089-5097.
Acknowledgements: NIL.
Disclosure of Interests: Huihua Ding: None declared, Chunde Bao: None declared, Jiankang Hu: None declared, Long Qian: None declared, Lei Yang: None declared, Zhongming Wang: None declared, Zili Fu: None declared, Ning Zhang: None declared, Changsong Lin: None declared, Cheng Zhao: None declared, Lingyun Sun: None declared, Rongshan Li: None declared, Wenli Chen: None declared, Hua Wei: None declared, Xiaoxia Yu: None declared, Juan Li: None declared, Haibing Chen: None declared, Yuan Liu: None declared, Zhiyong Chen: None declared, Xiaoyan Xu: None declared, Yuan Xue: None declared, Yongjun Mei: None declared, Dong Zhao: None declared, Rui Yan: None declared, Min Zhang: None declared, Bin Zhou: None declared, Jia Chen: None declared, Jing Liu: None declared, Zhenyu Jiang: None declared, Zhanqing Gu: None declared, Haoshu Cui Jiangsu Hengrui Pharmaceuticals Co., Ltd., Yanlin Ma Jiangsu Hengrui Pharmaceuticals Co., Ltd.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (