fetching data ... 
Background: Flares are common in rheumatoid arthritis (RA) and are sometimes preceded by changes in treatment. International recommendations advise using glucocorticoids (GC) primarily as bridging therapy until csDMARDs take effect to minimize the negative effects of prolonged use of GC:s [1]. Whether GC bridging therapy increases the risk of a subsequent flare, as defined by absolute changes in the CDAI score, has not been studied.
Objectives: To investigate the risk of flare following tapering and discontinuation of initial oral glucocorticoid therapy, and with initial glucocorticoid injections compared to bDMARD treatment in early RA.
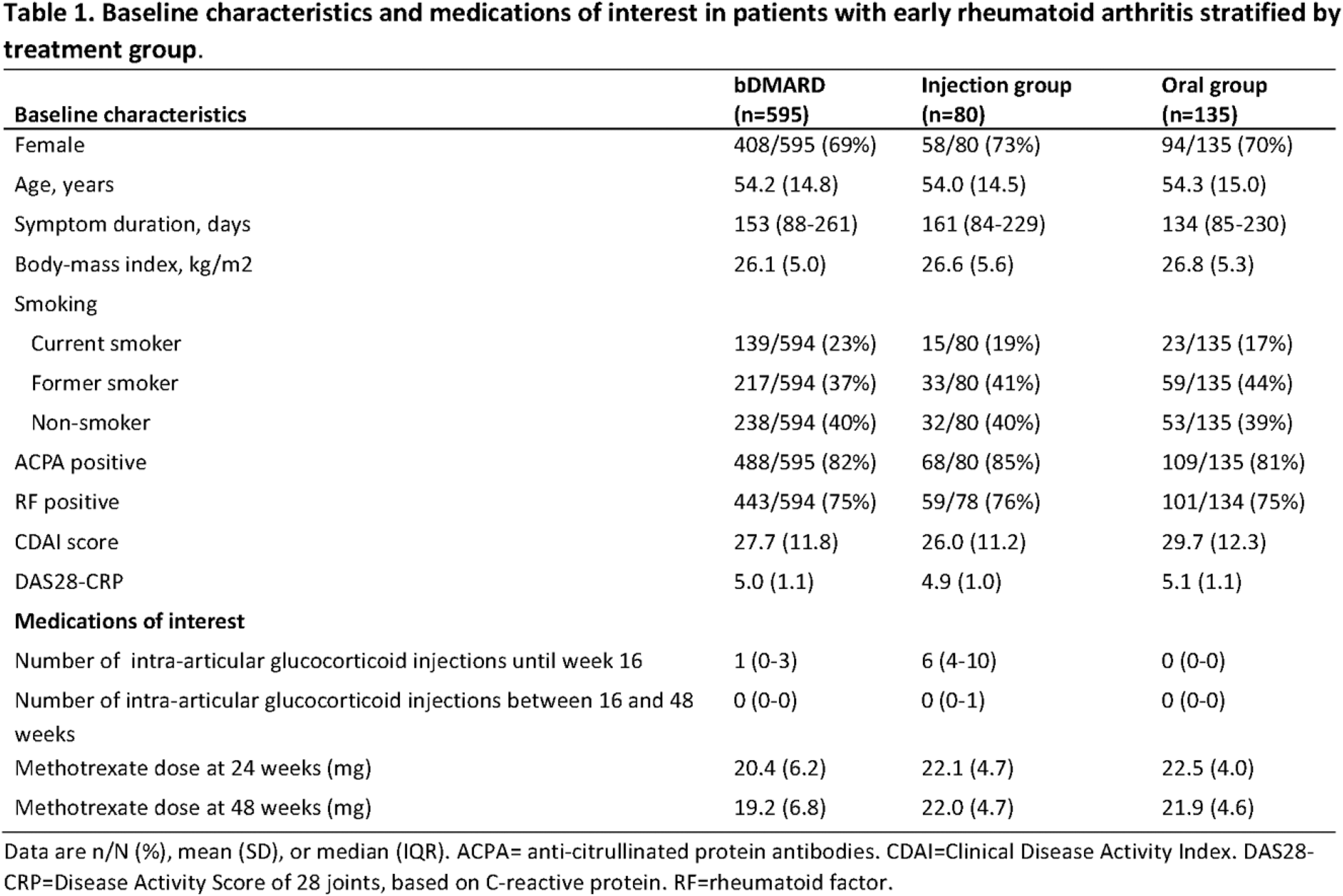
Methods: Data from the NORD-STAR trial, conducted in Sweden, Denmark, Norway, Finland, Netherlands, and Iceland, were used (NCT01491815) [2]. Clinical Disease Activity Index (CDAI) flare was defined as an increase of at least 4.5 units since the previous visit [3]. The NORD-STAR active conventional arm 1A (“Oral group”) received methotrexate plus oral glucocorticoids (started with 20 mg/day, tapered to 5 mg by week 9, and followed the protocol-prescribed discontinuation by week 36); The active conventional treatment 1B (“Injection group”) received triple therapy (methotrexate, sulfasalazine, hydroxychloroquine) and mandatory intra-articular glucocorticoid injections in swollen joints (maximum 4 joints or maximum 4 mL per visit). The bDMARD group received methotrexate plus one of the biologics (certolizumab pegol, abatacept, or tocilizumab). Intra-articular GC injections were allowed in all treatment groups when clinically indicated (except during weeks 20-24 and 44-48). The bDMARD group served as the reference for the oral group (with tapering and discontinuation) and for the injection group (no regimen changes). Flare rates were first analysed longitudinally using logistic generalized estimating equations (GEE). Additional analyses were performed for the oral subgroup of patients who discontinued glucocorticoids before 48 weeks with age, sex, and week-matched controls from bDMARD group and sex and week-matched patients from the injection group. This was done using logistic regression to assess the risk of flare at the visit following glucocorticoid discontinuation. Analyses were adjusted for sex, ACPA status, country, age, BMI, DAS28-CRP and smoking status at baseline.
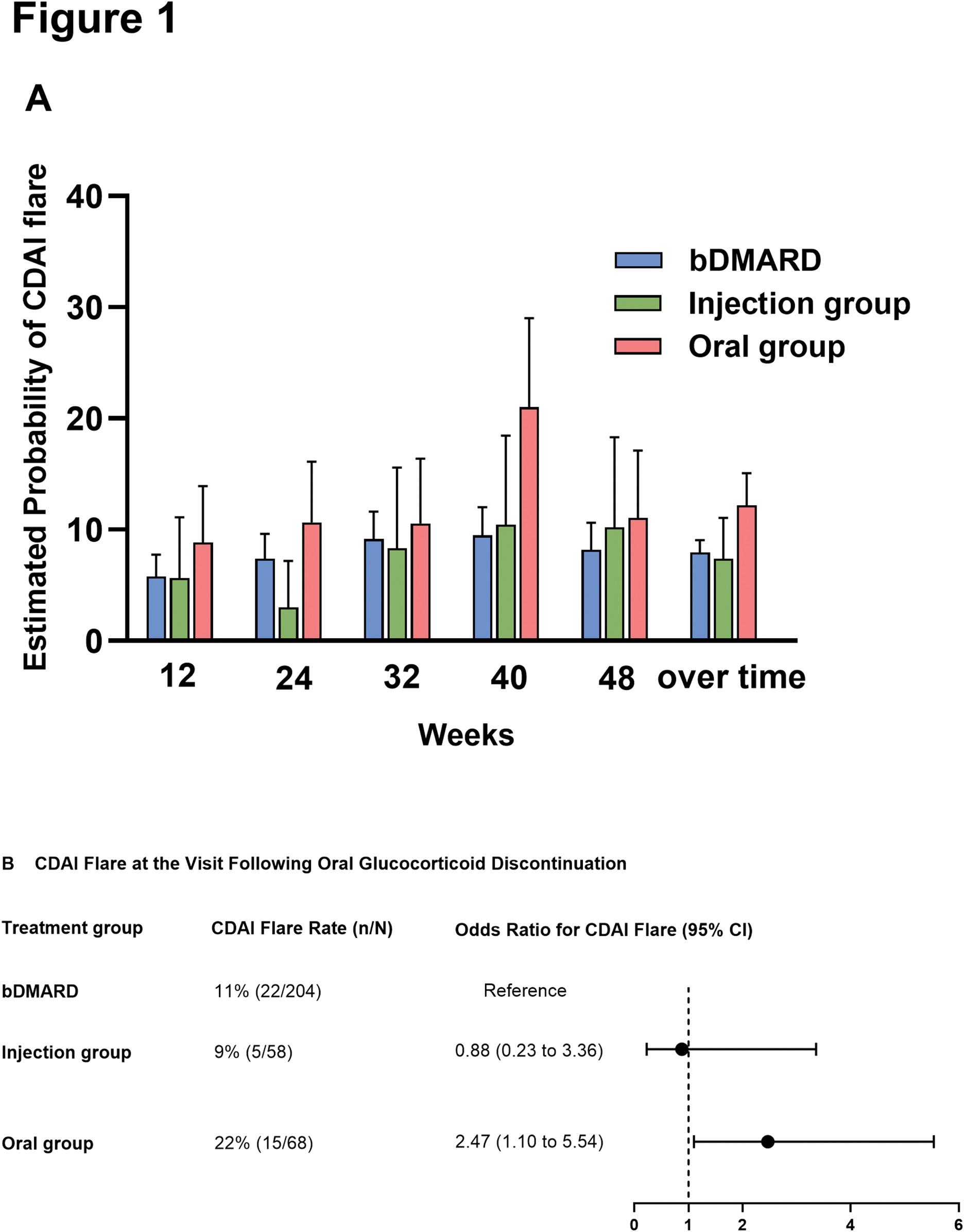
Results: A total of 810 randomised patients were included in this substudy: 135 in the oral group, 80 in the injection group, and 595 in the bDMARD group. During 48 weeks or until early termination, flares occurred at least once in 56/130 (43%) of the oral group, 18/75 (24%) of the injection group, and 160/565 (28%) of the bDMARD group patients. In the longitudinal GEE analysis, the risk of a CDAI-increase defined flare over time (at 12, 24, 32, 40, and 48 weeks) was higher in the oral group (OR: 1.62 [95% CI: 1.18-2.22]) than in the bDMARD group. When looking at individual time points, the risk was numerically higher at all visits and significantly higher at week 40 (OR: 2.58 [95% CI: 1.45–4.61]), the visit following protocol-prescribed discontinuation, compared to the bDMARD group. In contrast, patients treated with glucocorticoid injections had similar flare rates as the bDMARD group over time (OR: 0.92 [95% CI: 0.52-1.63], Figure 1A), despite majority of intra-articular injections being administered early in the study (Table 1). We observed that by 48 weeks, 71/135 (53%) patients in the oral group had discontinued glucocorticoids as planned and remained in the trial. Among these patients, the risk of flare was higher at the visit following glucocorticoid discontinuation (OR: 2.47 [95% CI: 1.10-5.54]) compared to matched bDMARD controls (Figure 1B).
Conclusion: Of the patients who discontinued oral glucocorticoids and remained in the trial at 48 weeks, the risk of a CDAI-defined flare was significantly higher after discontinuation of longer-term oral glucocorticoid bridging strategy, compared to bDMARD treatment. Initial intra-articular injections may have long-term effects, as injection group flare rates were similar to those of bDMARD treatment. When choosing longer-term, low-dose glucocorticoid bridging strategy for RA, the increased risk of a flare upon discontinuation must be considered.
REFERENCES: [1] Smolen, J.S., et al., EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis, 2023. 82 (1): p. 3-18.
[2] Østergaard, M., et al., Certolizumab pegol, abatacept, tocilizumab or active conventional treatment in early rheumatoid arthritis: 48-week clinical and radiographic results of the investigator-initiated randomised controlled NORD-STAR trial. Ann Rheum Dis, 2023. 82 (10): p. 1286-1295.
[3] Konzett, V., et al., Definition of rheumatoid arthritis flare based on SDAI and CDAI. Ann Rheum Dis, 2024. 83 (2): p. 169-176.
Acknowledgements: We express our gratitude to the patients, study nurses, investigators, joint assessors, data management and study teams who were involved in the NORD-STAR trial.
Disclosure of Interests: Kristina Lend: None declared, Jos W.R. Twisk: None declared, Frieda Koopman: None declared, Anna Rudin: None declared, Merete Lund Hetland Institutional grants from AbbVie, Bristol Myers Squibb, Eli Lilly, MSD, Pfizer, Sandoz, Novartis, Nordforsk and UCB; speaker honoraria from Medac, Novartis, Pfizer, Sandoz, and UCB; institutional data safety monitoring board or advisory board fees from AbbVie. MLH has chaired the steering committee of the Danish Rheumatology Quality Registry (DANBIO, DRQ), which receives public funding from the hospital owners and funding from pharmaceutical companies. MLH co-chairs EuroSpA, which generates real-world evidence of treatment of psoriatic arthritis and axial spondyloarthritis based on secondary data and is partly funded by Novartis and UCB, Till Uhlig speaker honoraria from Lilly, Pfizer, UCB and Galapagos, Dan Nordström Bristol Myers Squibb, Lilly, Novartis, Pfizer, and UCB, Research grant from MSD; speaker honoraria from Pfizer and UCB; participation on a data safety monitoring board or advisory board fees from UCB, Michael Nurmohamed: None declared, Bjorn Gudbjornsson: None declared, Kim Hørslev-Petersen: None declared, Marte S Heiberg: None declared, Tuulikki Sokka-Isler: None declared, Gerdur Grondal: None declared, Espen A Haavardsholm personal speaker honoraria from Pfizer, UCB, and Novartis; and participation on a data safety monitoring board or advisory board fees from AbbVie, Pfizer, and Eli Lilly, Mikkel Østergaard Abbvie, BMS, Boehringer-Ingelheim, Celgene, Eli-Lilly, Galapagos, Gilead, Hospira, Janssen, Merck, Novartis, Pfizer, Sandoz, and UCB, Research grants from AbbVie, Amgen, BMS, Merck, Celgene, Eli Lilly, Novartis, and UCB, speaker fees from Abbvie, BMS, Boehringer-Ingelheim, Celgene, Eli-Lilly, Galapagos, Gilead, Janssen, MEDAC, Merck, Novartis, Pfizer, Sandoz, and UCB, Jon Lampa: None declared, Ronald F. van Vollenhoven AbbVie, AstraZeneca, Biogen, Bristol Myers Squibb, Galapagos, GSK, Janssen, Pfizer, RemeGen, and UCB, Institutional grants for research or education from Alfasigma, AstraZeneca, Bristol Myers Squibb, Galapagos, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (