fetching data ... 
Background: Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare form of systemic necrotizing small vessel vasculitis associated with anti-neutrophil cytoplasmic antibodies (ANCA). Rheumatoid factor (RF) is an autoantibody directed against the Fc portion of immunoglobulin G (IgG) that can be found in the serum of patients affected with rheumatoid arthritis and other autoimmune and non-autoimmune conditions, as well as in healthy subjects. The presence of RF has been reported in 35-45% of patients with EGPA.
Objectives: The aim of this study is to investigate RF positivity at the time of diagnosis and to evaluate its prognostic value in predicting vasculitic relapses in EGPA.
Methods: We reviewed consecutive patients newly diagnosed with EGPA between January 1992 and September 2024 who were referred to our Vasculitis Center. Patients were included if they had undergone RF assessment at diagnosis and had a minimum follow-up of 12 months. Clinical and serological data were collected at baseline, during each vasculitic relapse, and at the final follow-up. Relapse was defined as the new onset, reappearance, or worsening of systemic symptoms (excluding asthma and otolaryngological symptoms) and a Birmingham Vasculitis Activity Score version 3 (BVASv3) > 0. Descriptive statistics (medians, percentages, and interquartile ranges) summarized cohort characteristics. The Wilcoxon test was used for continuous variables, and the Pearson chi-square test for categorical variables. P-values were adjusted for multiple comparisons using the Benjamini-Hochberg-Yekutieli correction. To identify relapse risk patterns in EGPA patients, a random forest model (using the ‘randomForestSRC’ package in R) was applied. The algorithm combines decision trees with bootstrap aggregating (bagging) (approximately 63% of the total sample size), forming an ensemble model for greater accuracy and reduced overfitting. The model trains 10,000 trees on random subsets, selecting 6 variables out of the total predictors. Multiple imputation (three imputations per run) was used to handle missing data and reduce bias. Variable importance scores (VIMP) indicated each predictor’s contribution to the model, while Shapley values interpreted individual predictions and overall model performance.
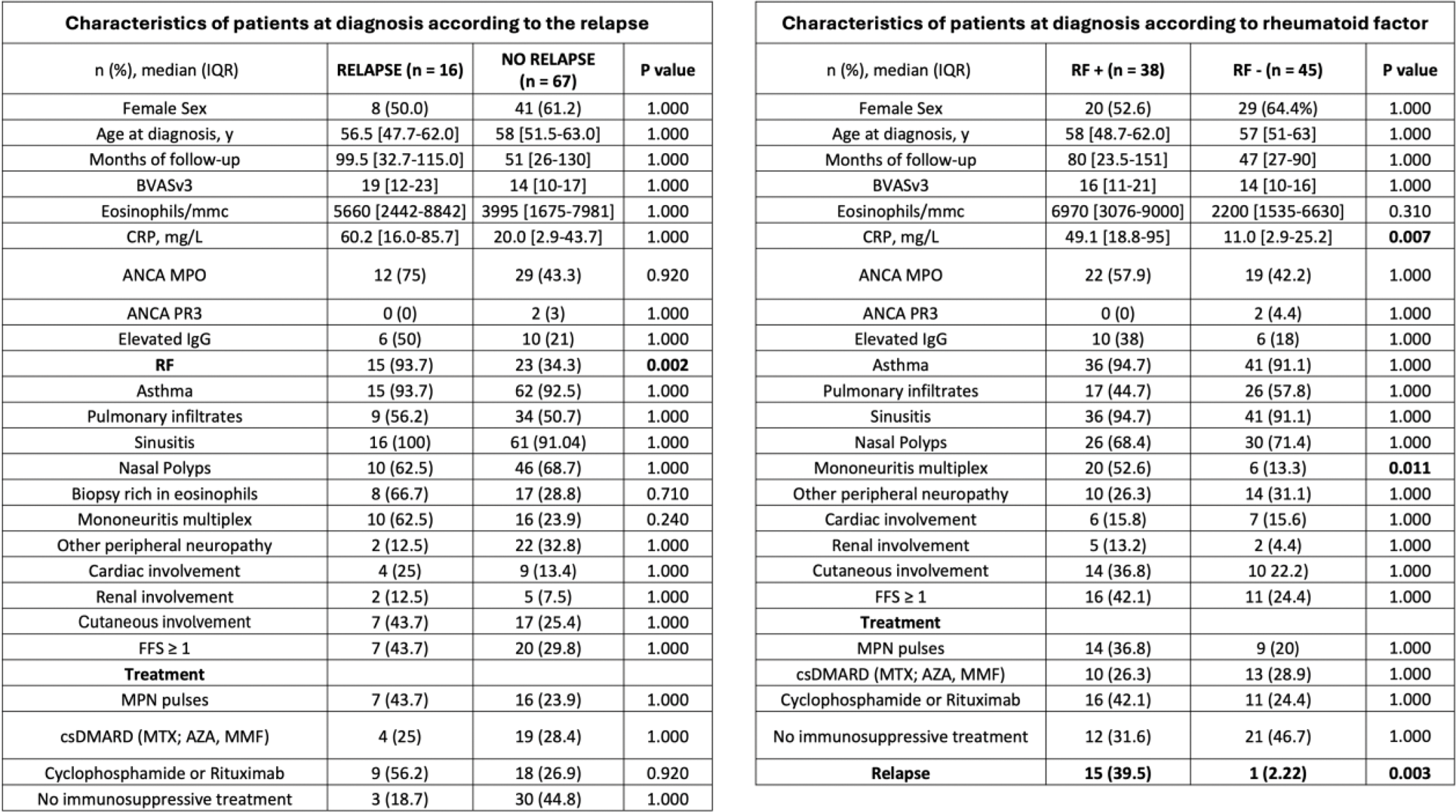
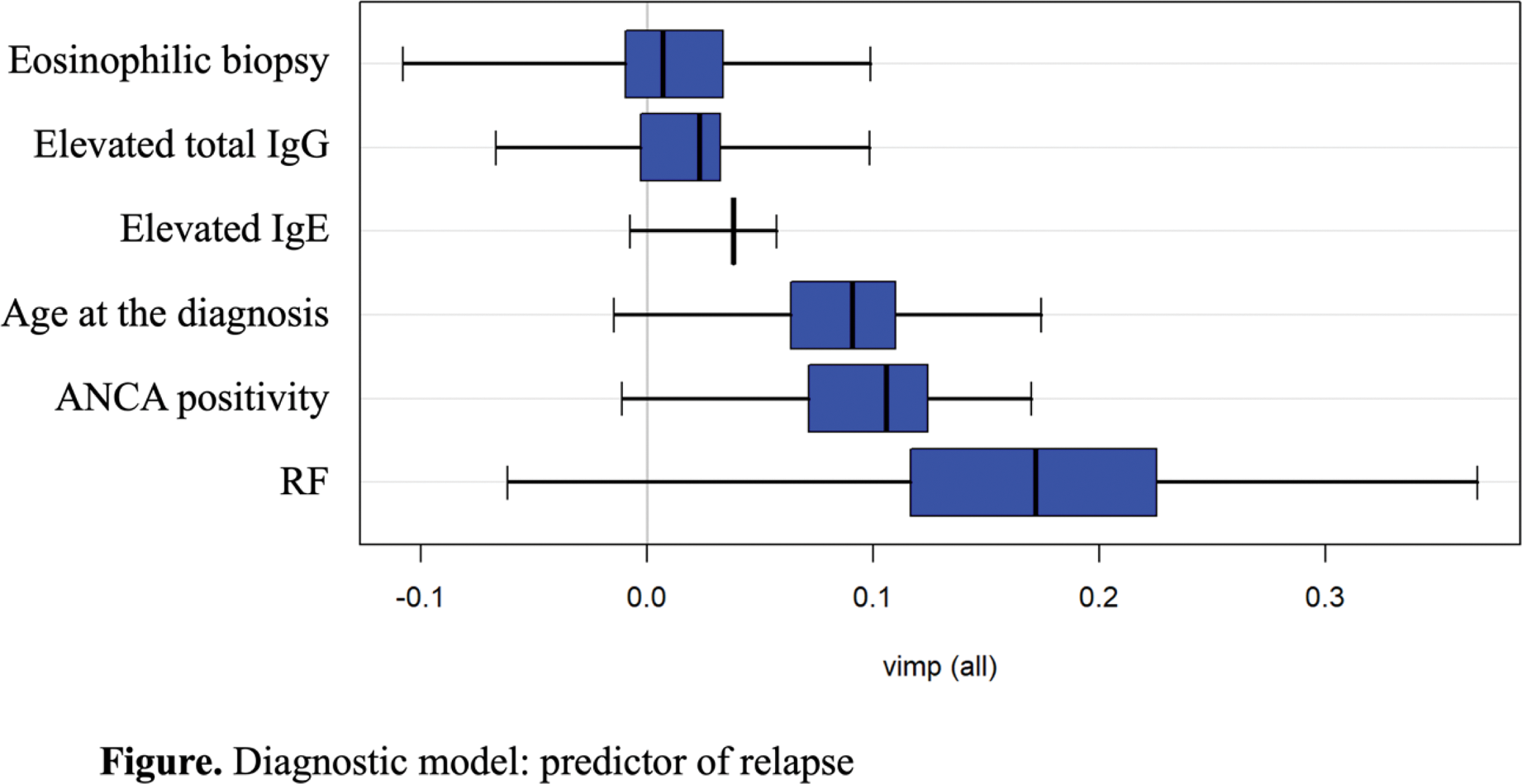
Results: A total of 83 patients classified with EGPA according to the 2022 ACR/EULAR classification criteria were included: 38 were RF positive (RF+) and 45 were RF negative (RF-) at diagnosis. The median follow-up was 80 [IQR: 23.5-151] months for the RF+ group and 47 [27-90] months for the RF- group, with no significant difference between the groups (p=1.000). At diagnosis, the groups significantly differed in CRP levels (49.1 [18.8-95] vs. 11.0 [2.9-25.2], p=0.007) and the presence of mononeuritis multiplex (20 [52.6%] vs. 6 [13.3%], p=0.011). The RF+ group had a significantly higher vasculitic relapse rate compared to the RF- group (15/38 [39.5%] vs. 1/45 [2.2%], p=0.003). The median time to relapse was 29 [11.8-71.8] months. Notably, patients in the RF+ group more frequently received methylprednisolone pulses (14 [37.8%] vs. 9 [18.3%]) and cyclophosphamide and/or rituximab (16 [43.2%] vs. 11 [22.5%]) at baseline compared to the RF- group. The study revealed that 67 patients did not experience any relapse, while 16 patients experienced at least one relapse. The Random Forest model, applied to the cohort of 83 patients (67 non-relapsers and 16 relapsing), identified the variable RF (VIMP 0.2031, 95%CI -0.012 to 0.307) as the most significant predictor of relapse, contributing significantly to the model, despite the wide confidence interval, suggesting some variability at the lower end. Variables like ANCA (VIMP 0.0656, 95%CI 0.016 to 0.160) and age at disease onset (VIMP 0.0530, 95%CI 0.009 to 0.155) were identified as moderately important predictors. Conversely, elevated IgE (VIMP 0.0203, 95%CI 0.002 to 0.056) and elevated IgG (VIMP 0.0124, 95%CI -0.050 to 0.077) had minimal impact on the model’s predictive performance of relapse. The model attained a sensitivity of 96.3%, a specificity of 89.3%, and an F1 score of 88.1%. The misclassification rate was 21.7%, with an AUC of 0.8078, indicating a strong ability of the model to distinguish between the two classes (relapse vs. non-relapse). When evaluating the contribution of each feature to the prediction using the Shapley value (phi) method, the absence of RF strongly increased the predicted probability of being a non-relapser (phi +0.1469). The presence of ANCA and older age at disease onset slightly increased the likelihood of relapse (phi -0.0270 and -0.0133, respectively). Features such as extravascular eosinophilic inflammation on biopsy and elevated total serum IgG also contributed positively, though their influence was relatively minor (phi +0.0178 and +0.0193, respectively). Elevated serum IgE had only a minimal effect on the prediction (phi -0.0007).
Conclusion: This study highlights the significant prognostic role of RF in predicting vasculitic relapses in EGPA patients. The random forest model identified RF presence as the most important relapse predictor, with a high variable importance score, despite some variability in its confidence interval. Other moderately important predictors included ANCA positivity and age at disease onset. RF positivity at diagnosis is a critical prognostic factor for relapse, highlighting the importance of early identification and tailored treatment strategies for RF-positive patients.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (