fetching data ... 
Background: Psoriatic arthritis (PsA) is a complex inflammatory disease with variable clinical manifestations affecting joints and entheses within the peripheral and central skeleton. Clinical and composite clinico-biological scoring systems such as CASPAR, TJC (Tender Joint Count), SJC (Swollen Joint Count) and DAPSA are used to evaluate the disease severity and the response to treatment. Implementation of imaging assessments such as the Whole-Body MRI (WB-MRI) Score for Inflammation in Peripheral Joints and Entheses (MRI-WIPE) may improve disease monitoring and evaluation of treatment response [1].
Objectives: This study compares WB-MRI findings with clinic-biological assessments to evaluate treatment response in patients with PsA treated with adalimumab, guselkumab, or ustekinumab.
Methods: Between December 2019 and August 2023, 32 PsA patients were enrolled in the TIGERS study (TNF and IL23 blocking agents Gene Expression Ratios in the Psoriatic Arthritis Synovium Study) (registered as NCT04261010; EudraCT 2017-003249-1). Patients were randomly assigned to one of three treatment arms: adalimumab (TNF inhibitor), guselkumab (IL-23p19 inhibitor) and ustekinumab (IL-23 inhibitor). All underwent WB-MRI examinations covering the body from the cervico-occipital junction to the toes, and including Short Tau Inversion Recovery (STIR) and post-contrast T1 Dixon sequences optimized for the axial and peripheral skeletal skeleton. WB-MRI studies were assessed at baseline and at six months using the MRI WIPE system [1] which was further complemented by assessment of the spine, sacroiliac joints, and tenosynovitis of the wrists and ankles. Clinico-biological outcomes (TJC68, SJC66, DAPSA, Leeds Enthesitis index) were measured. Statistical analyses included Kruskal-Wallis, Wilcoxon, and Spearman’s rho tests.
Results: Patient characteristics and baseline disease scores are shown in Table 1. Post-treatment clinico-biological and imaging scores and differences from baseline scores are shown in Table 2. Only adalimumab significantly reduced imaging scores at 6 months (MRI WIPE: median decrease = -39 units; Joint synovitis score: median decrease = -23 units). Modest improvements in some imaging scores observed with guselkumab did not reach statistical significance. All treatments significantly reduced clinical indices of disease activity as reflected by the change in SJC66 (median decrease ranging from -9.5 to -3.0 units) and DAPSA (median decrease ranging from -31 to -5.8 units). A strong correlation (rho = 0.78, p = 0.023) was observed between changes in the clinical SJC66 and changes in the MRI joint synovitis score.
Conclusion: This study highlights the promising role of combining WB-MRI with clinical assessment in the management of PsA. While all three biologics demonstrated clinic-biological efficacy in reducing disease activity, adalimumab was the most effective in reducing the disease burden as measured by imaging. WB-MRI, using recommended comprehensive scoring systems such as MRI-WIPE, can identify subclinical or deep unassessable disease activity and provide unique insight into treatment response. It offers the prospect of refining the differential assessment of the efficacy of new treatments and for guiding personalized therapeutic strategies in the management of PsA.
REFERENCES: [1] Krabbe S et al.; OMERACT MRI in Arthritis Working Group. Development and Validation of an OMERACT MRI Whole-Body Score for Inflammation in Peripheral Joints and Entheses in Inflammatory Arthritis (MRI-WIPE). J Rheumatol. 2019 Sep;46(9):1215-1221. doi: 10.3899/jrheum.181084. Epub 2019 Feb 15. PMID: 30770508.
Table 1. Baseline patient demographics and disease characteristics (95%CI are given into brackets) in the whole patient population and in the three therapeutic arms. No significant differences in these parameters were observed between the different treatment arms.
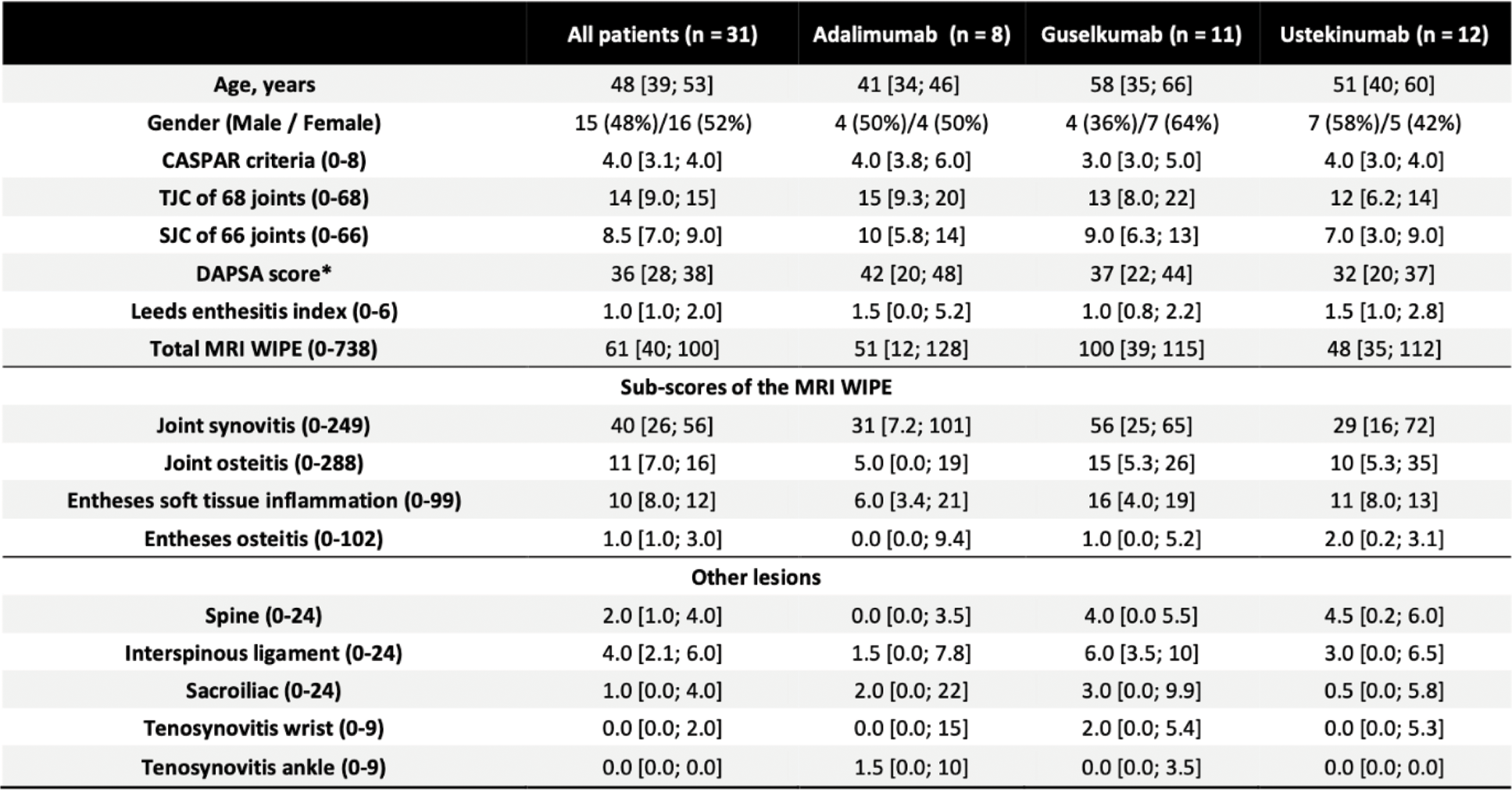
Abbreviations: CASPAR: Classification Criteria for Psoriatic Arthritis; TJC: Tender Joint Count of 68 joints; SJC: Swollen Joint Count of 66 joints; DAPSA: Disease Activity in Psoriatic Arthritis score; MRI WIPE: MRI Whole-Body Score for Inflammation in Peripheral Joints and Entheses in Inflammatory Arthritis
*DAPSA score: ≤4 (Remission), >4–≤14 (Low Disease Activity), >14–≤28 (moderate disease activity) and >28 (high disease activity)
Table 2. Median differences between pre and post treatment scores (computed as the difference = “score 6 months - score baseline ”) assessed using Wilcoxon paired test (95%CIs are given into brackets). After Bonferroni correction, statistical significance was declared at p < 0.017. The table reads as follows. In the patients group treated with adalimumab (second line, left column), a lower TJC68 score was observed at 6 months (median decrease = -13 units, p = 0.016). In the patients group treated with guselkumab (first line, middle column), a lower TJC68 score was observed at 6 months (median decrease = -8.0 units, p = 0.001). In the patients group treated with ustekinumab (second line, right column), no difference was observed ( p = 0.078). Imaging score Joint synovitis significantly decreased at 6 months with adalimumab, but not with both other treatments (median decrease of -23 units). The score MRI WIPE (resulting from the sum of the 4 previous scores) also decreased at 6 months with adalimumab (median decrease of -39 units).
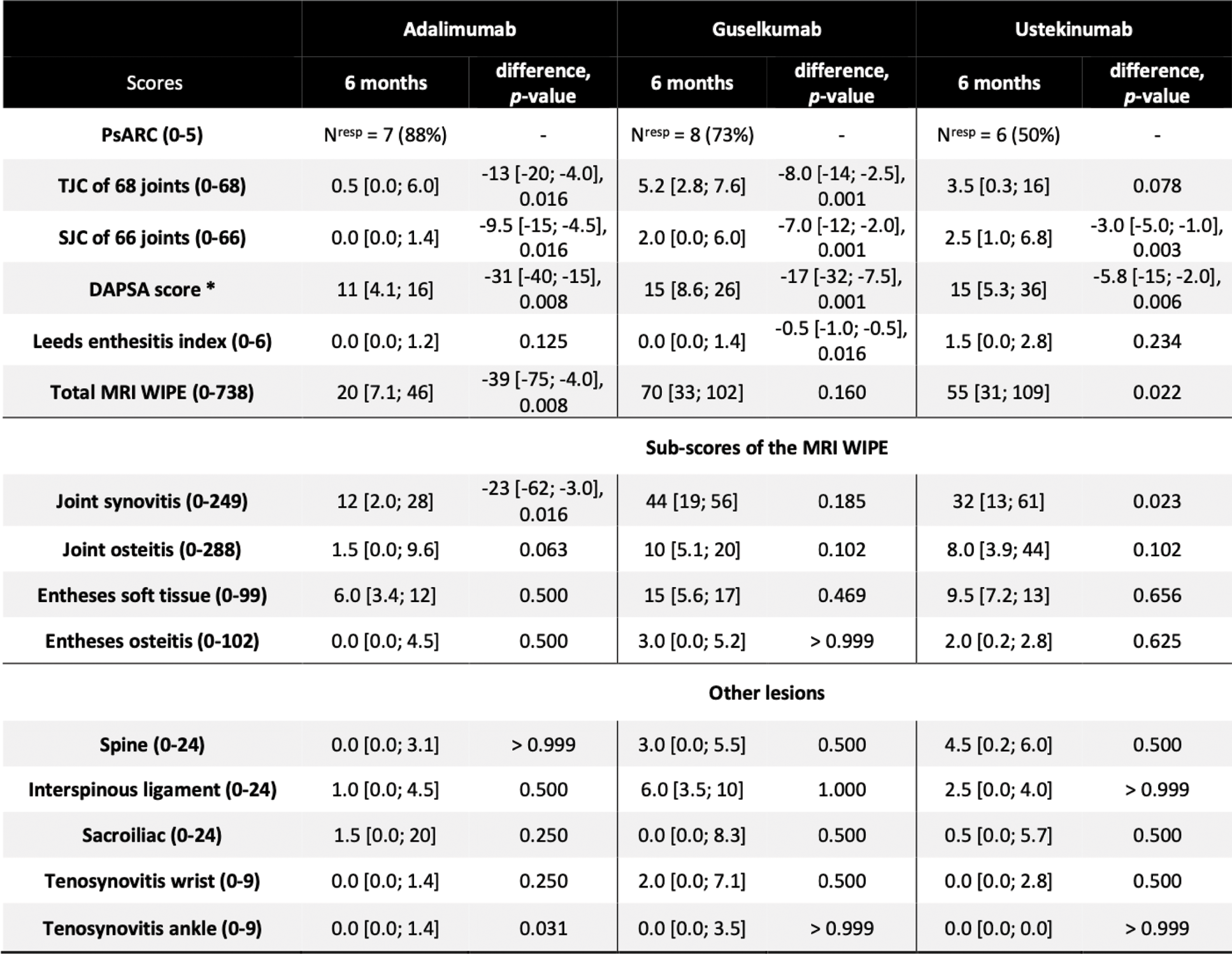
Abbreviations: PsARC: Psoriatic Arthritis Response Criteria; TJC: Tender Joint Count of 68 joints; SJC: Swollen Joint Count of 66 joints; DAPSA: Disease Activity in Psoriatic Arthritis score; MRI WIPE: MRI Whole-Body Score for Inflammation in Peripheral Joints and Entheses in Inflammatory Arthritis
*DAPSA score: ≤4 (Remission), >4–≤14 (Low Disease Activity), >14–≤28 (moderate disease activity) and >28 (high disease activity)
Acknowledgements: NIL.
Disclosure of Interests: Caroline Chabot: None declared, Pauline Krug: None declared, Anthony Lichaa: None declared, Nicolas Michoux: None declared, Gaëtan Duchêne: None declared, Adrien Nzeusseu Toukap Janssen, Eli-Lilly, UCB, Abbvie, Novartis, Janssen, Amgen, Frédéric E. Lecouvet: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (