fetching data ... 
Background: Although Janus kinase (JAK) inhibitors have established a novel treatment approach for rheumatoid arthritis (RA) in real-world clinical practice, achieving the primary treat-to-target (T2T) goal remains challenging for many patients.
Objectives: (i) To identify predictive factors associated with achieving remission or low disease activity at the first 6 months of JAK inhibitor treatment. (ii) To determine whether the predictive factors identified linked to the achievement of the T2T goal at the first 6 months, also contribute to differences in the long-term effectiveness of JAK inhibitor treatment.
Methods: This is an observational, retrospective study that involves RA patients receiving tofacitinib, baricitinib, upadacitinib, or filgotinib between 2017 and 2025. Potential predictive factors taken into account were sociodemographic [age, sex, body mass index (BMI)], anamnesis (RA disease duration), RA disease activity (assessed through Clinical Disease Activity Index), seropositivity [rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies], JAK inhibitor selectivity, number of prior RA treatments [previous conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), previous biologic DMARDs (bDMARDs), and previous JAK inhibitors], type of previous bDMARDs (tumor necrosis factor-alpha inhibitor, interleukin 6 inhibitor, abatacept, rituximab, and anakinra), and concomitant RA treatments (presence or absence of csDMARDs). Predictive factors of achieving the T2T goal at 6 months were identified through logistic regression analyses. Disparities in the treatment effectiveness retention based on predictive factors were assessed using the Kaplan-Meier estimate and compared with the log-rank test.
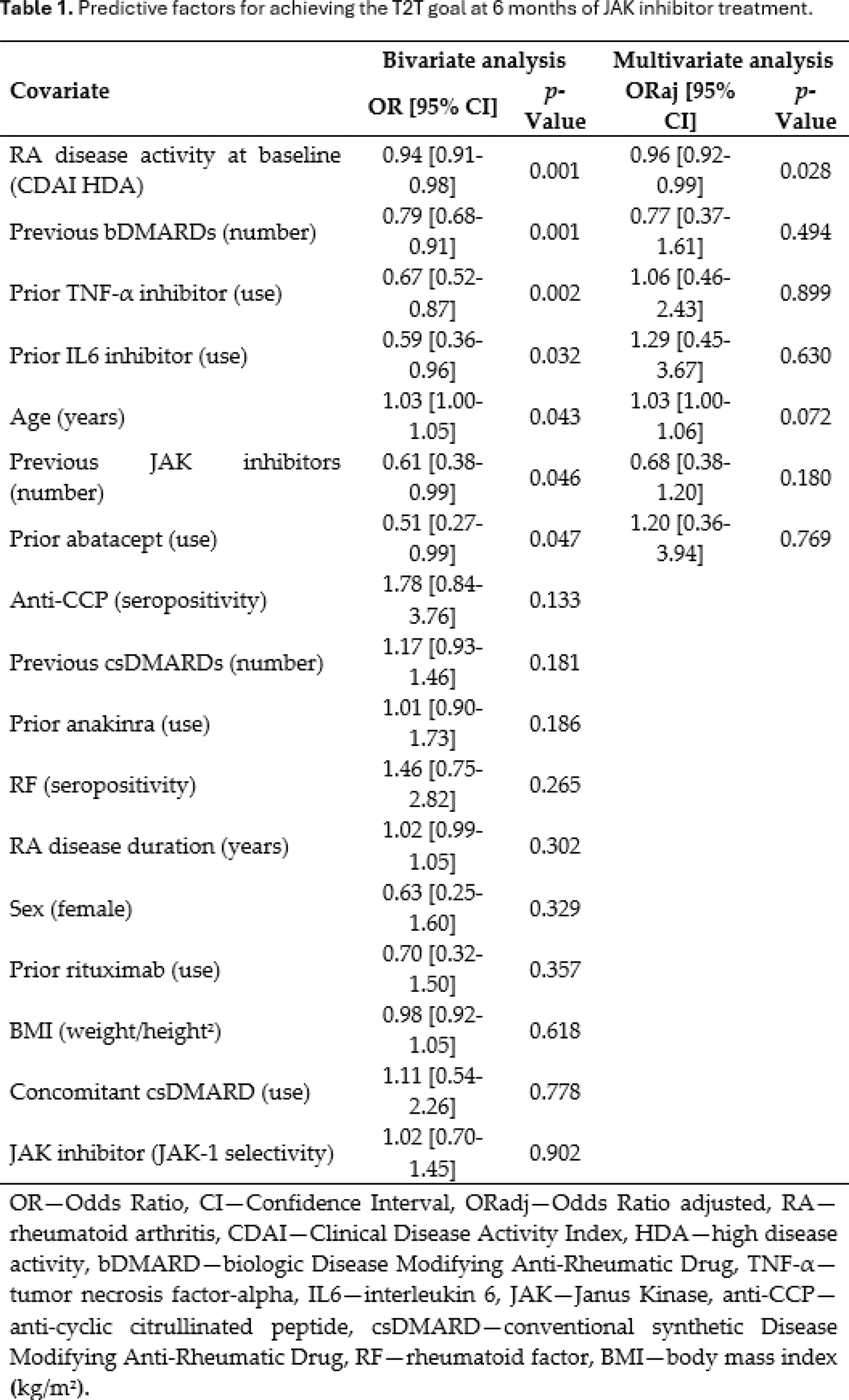
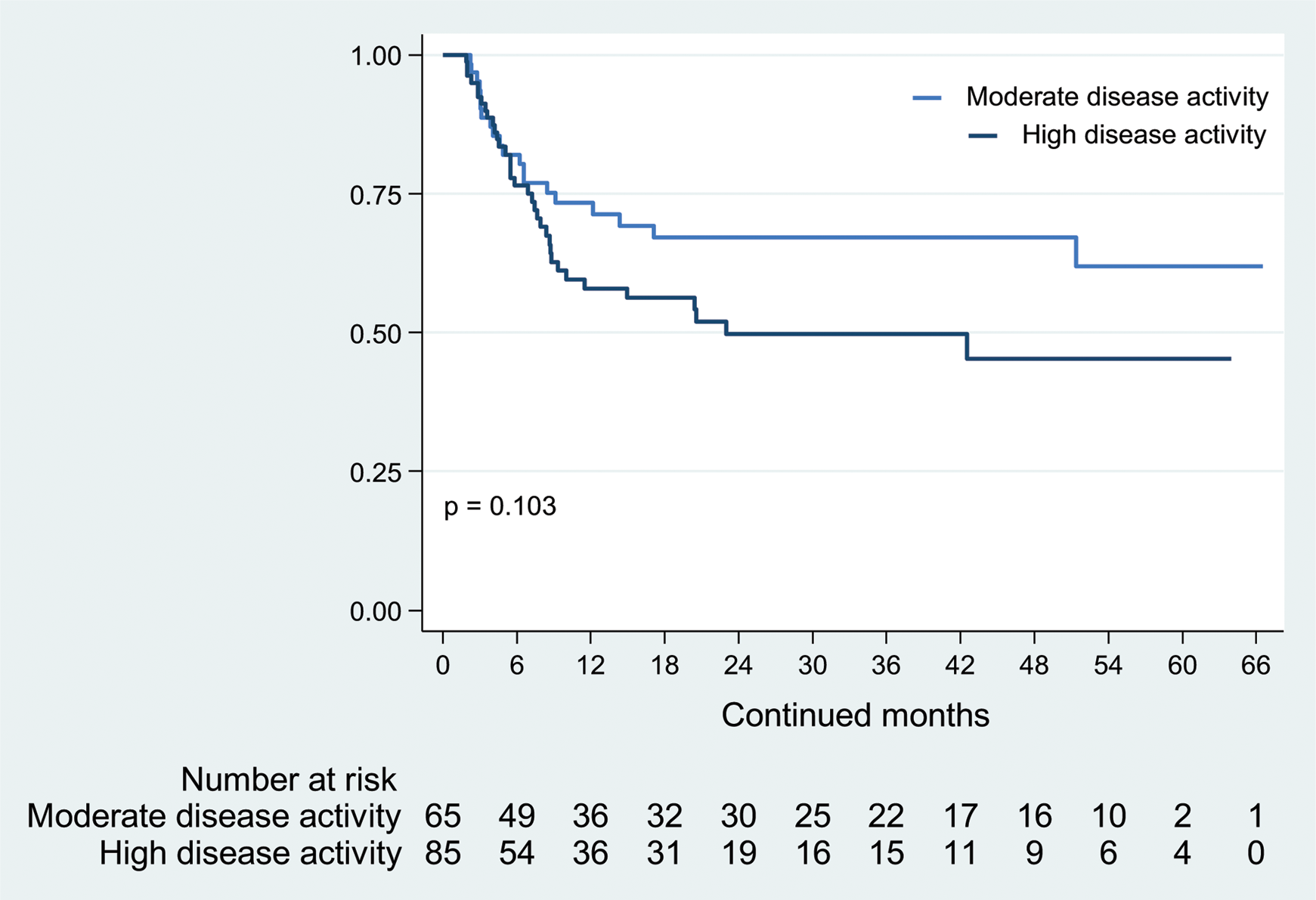
Results: One hundred fifty patients were included: 81 (54%) T2T achievers and 69 (46%) T2T non-achievers. High disease activity at baseline, with respect to moderate activity, was identified as an unfavorable factor for achieving the T2T goal (Odds ratio adjusted: 0.96; 95% confidence interval: 0.92-0.99; p =0.028; Table 1). In treatment effectiveness retention rates, no differences were observed between patients with high versus moderate disease activity ( p =0.103; Figure 1).
Conclusion: In RA, high disease activity at the initiation of treatment with tofacitinib, baricitinib, upadacitinib, or filgotinib does not preclude an effective treatment response but is associated with an increased risk of therapeutic failure. Factors not related to the achievement of the T2T goal at 6 months of JAK inhibitor treatment include: age, female sex, BMI, RA disease duration, seropositivity for RF, seropositivity for anti-CCP, JAK inhibitor selectivity, type and number of prior bDMARDs, concomitant use and number of prior csDMARDs, and number of prior JAK inhibitors.
REFERENCES: NIL.
JAK inhibitor retention due to lack of treatment effectiveness.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (