fetching data ... 
Background: Systemic Lupus Erythematosus (SLE)-related joint involvement can be identified in up to 90% of patients during the disease course. Recently, several papers tried to unveil the ultrasound (US) appearance of SLE joint involvement, as previously done for Rheumatoid Arthritis (RA): it is usually underestimated in its prevalence and severity, and it can progress towards chronic disease and bone erosions.
Objectives: In the present study, by applying a multi-statistical approach, we aimed to detect any clusters for severity and distribution of US-detected joint inflammation in SLE-related joint involvement.
Methods: SLE patients were enrolled according to the 2019 ACR/EULAR Criteria with active or previous history of joint involvement. The US was performed at the level of knees, wrists, metacarpophalangeal (MCPs), proximal interphalangeal (PIPs), and metatarsophalangeal (MTPs) joints. The synovitis gray-scale (GS) and Power Doppler (PD) were scored using the scoring system proposed by the EULAR-OMERACT ultrasound task force. Principal Component Analysis (PCA) and Unsupervised Hierarchical Cluster Analysis (CA) [with application of Euclidean distance and Ward agglomerative method] were performed to define the presence of clusters. Spearman r coefficient was applied for correlation analysis. As control for the ultrasound assessment, we evaluated a cohort of RA patients.
Results: We included 119 SLE patients (M/F 8/111; median age 50.1 years, IQR 16.7; median disease duration 162 months, IQR 204). As control, we enrolled 135 RA patients (M/F 99/36; median age 58 years, IQR 15.5; median disease duration 96 months, IQR 141.0). In the SLE cohort, we evaluated 4046 joints: among these, 375 joints (9.3%) showed at least a US-Grade 1 synovitis. The prevalence for each joint was graphically represented in Figure 1. The radiocarpal joint in the wrist was the most commonly involved by synovitis, with a prevalence of any grade synovitis of 63.5% in the right (R) joint and 54.2% for left (L), followed by the knees (R 20.3%, L 18.6%), 2MCP and 4MCP (R 11.86, L 9.32 for both joints), and 1MTP (R 11.86, L 11.02). Only nineteen-six joints (2.3%) had at least Grade ≥2 synovitis, mainly at the level of the radiocarpal joint (R 8.40%, L 7.56%), and knees (R 6.72%, L 5.8). Bone erosions (BE) were identified in 76 joints, with a cumulative higher prevalence at MCPs than in other joints. We applied PCA on US-detected synovitis to assess joints prone to be concurrently involved in individuals by using visual clusters. Indeed, we found four apparent clusters, representing different anatomical sites: the first (black) with the involvement of medium-large joints (wrists and knees), a second one (red) involving metatarsophalangeal joints, the third (orange) interphalangeal joints, and the fourth one (green) metacarpophalangeal joints (Figure 2A). Moreover, we built a correlation matrix to demonstrate the association between the presence of US-detected synovitis in each single joint. Each single cell in Figure 2B represents the r Spearman value for the correlation between synovitis detection in every possible correlation. According to the strength of the correlation, it was possible to confirm the presence of four different clusters as following: MCPs, PIPs, knees, and wrists (Figure 2B). Through an unsupervised cluster analysis, we identified four different clusters of US synovitis. The involvement of MCPs joints was identified as a specific cluster; knee and wrist were aggregated in a specific cluster. Differently from the previous analysis, 1MTP identified a different cluster, while PIPs and MTPs were combined into the same cluster. Finally, we performed a comparison between SLE and RA patients in terms of US-detected findings. As expected, RA patients showed a higher number of joints with US-detected synovitis compared with SLE patients (12.8% versus 9.3%; p<0.0001). However, when considering each joint separately, a statistical difference was found only for 2MTP (p<0.001), 1MTP (p=0.004) and 3MTP (p < 0.0001). As expected, the prevalence of bone erosions was significantly higher in RA compared to SLE (p<0.0001).
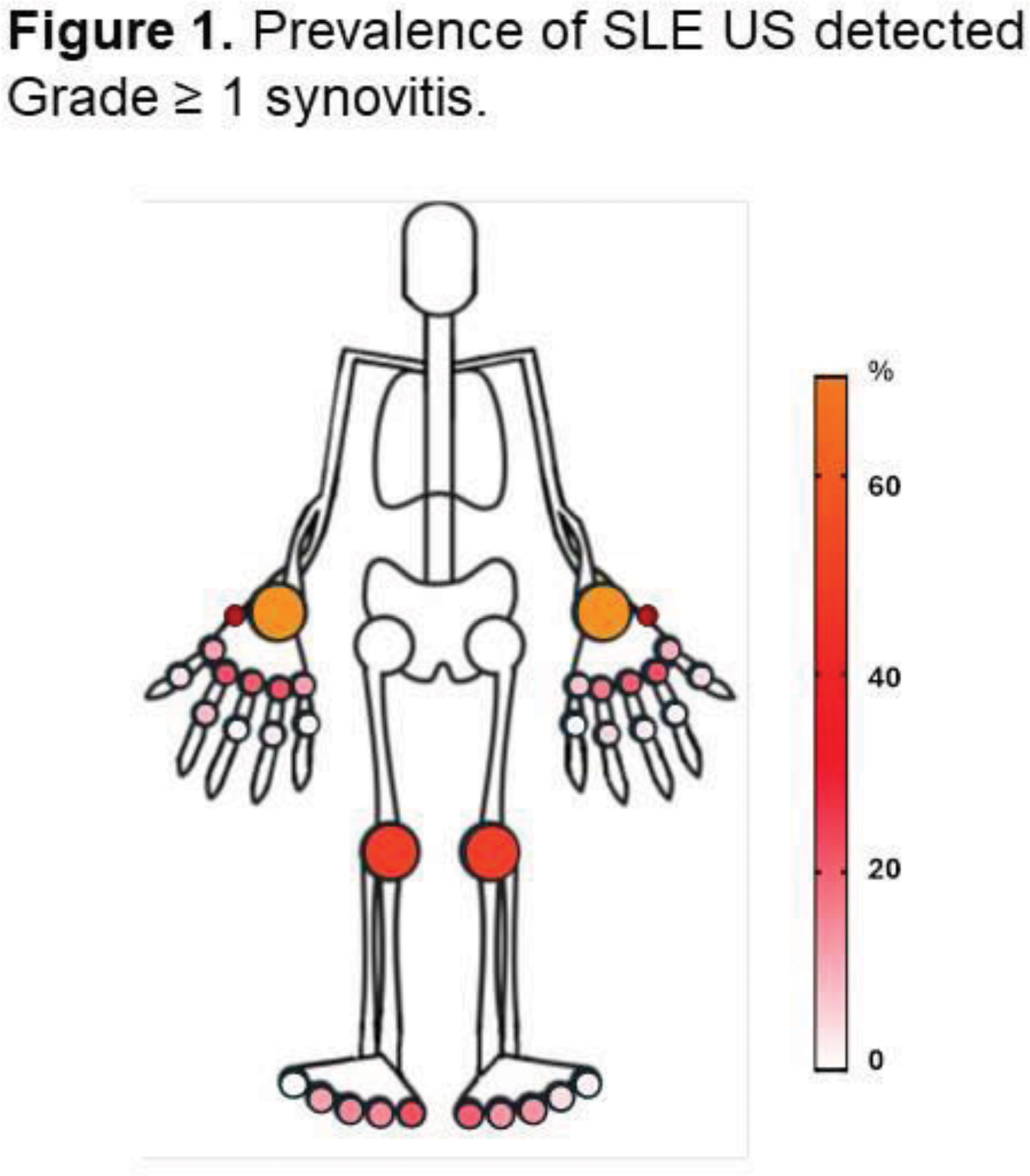
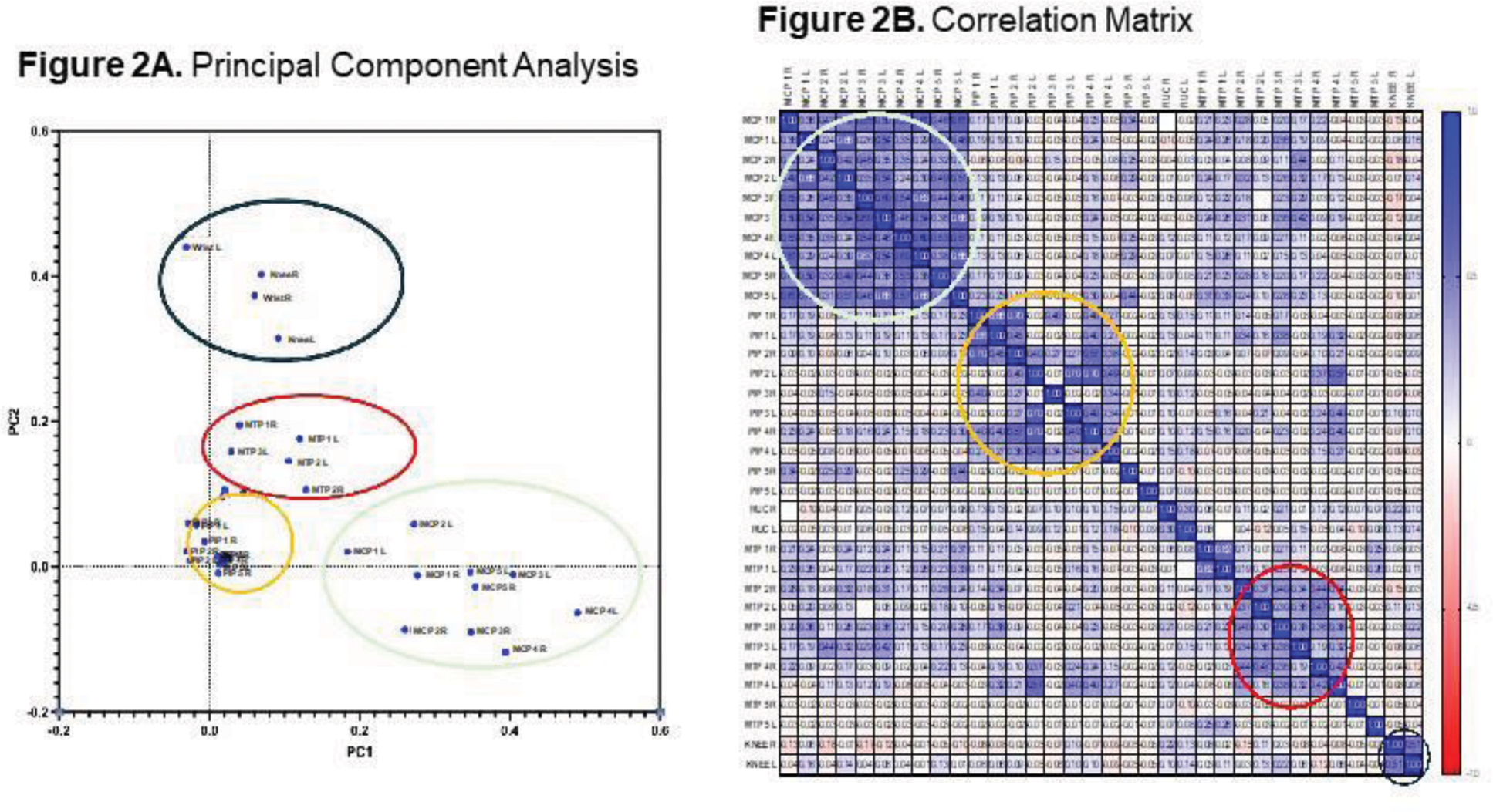
Conclusion: Wrists and knees were the most commonly involved joints according to US assessment, followed by MCPs. Through a multi-statistical approach, we demonstrated the presence of at least three different US-detected clusters: the “MCPs” Cluster, the “IFPs/MTPs” Cluster, and the “medium-joint” Cluster (including knees-wrists).
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (