fetching data ... 
Background: Musculoskeletal ultrasound (US) could help identify D2TRA patients through persistent joint inflammation. However, there is a need for reliable US patterns for risk stratification before meeting D2TRA criteria, which has important clinical implications [1].
Objectives: To investigate US findings and predictors of D2TRA1 and to characterize clinical features of D2T patients in a monocentric cohort.
Methods: Patients with D2TRA seen at our clinic between 2020-2024 were retrospectively enrolled in this study. Demographic, US and clinical data were collected and compared with a group of consecutive non-D2TRA patients followed up at our clinic across the same timespan. Patients displaying >5% of missing data records were excluded from the study. We considered as index US the one performed in patients naïve to b/tsDMARDs. The following areas were evaluated by US: wrists, metacarpophalangeal joints (MCP), proximal interphalangeal joints (PIP), shoulders, knees and ankles. All US assessments were performed by expert rheumatologists from our center using an Esaote MyLabX8 ultrasound machine with a high-resolution 15-24 MHz linear probe and assessed according to OMERACT criteria for synovitis, erosions and tenosynovitis [2]. A standardized and internationally approved scanning technique was used for the assessment of the different joint sites [3]. Chi-square test, Fisher, Wilcoxon test and T-test were used for statistical analysis as needed.
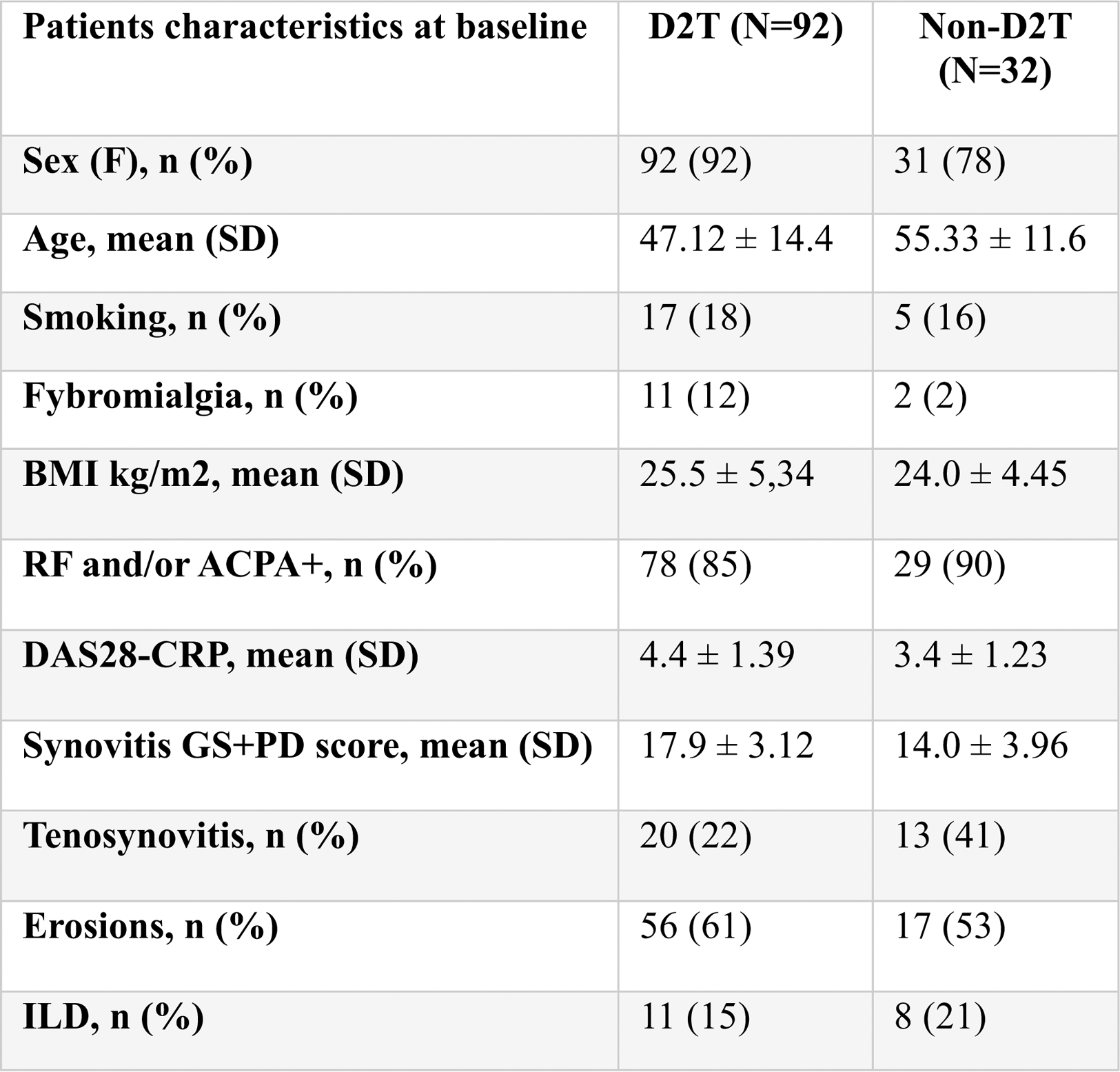
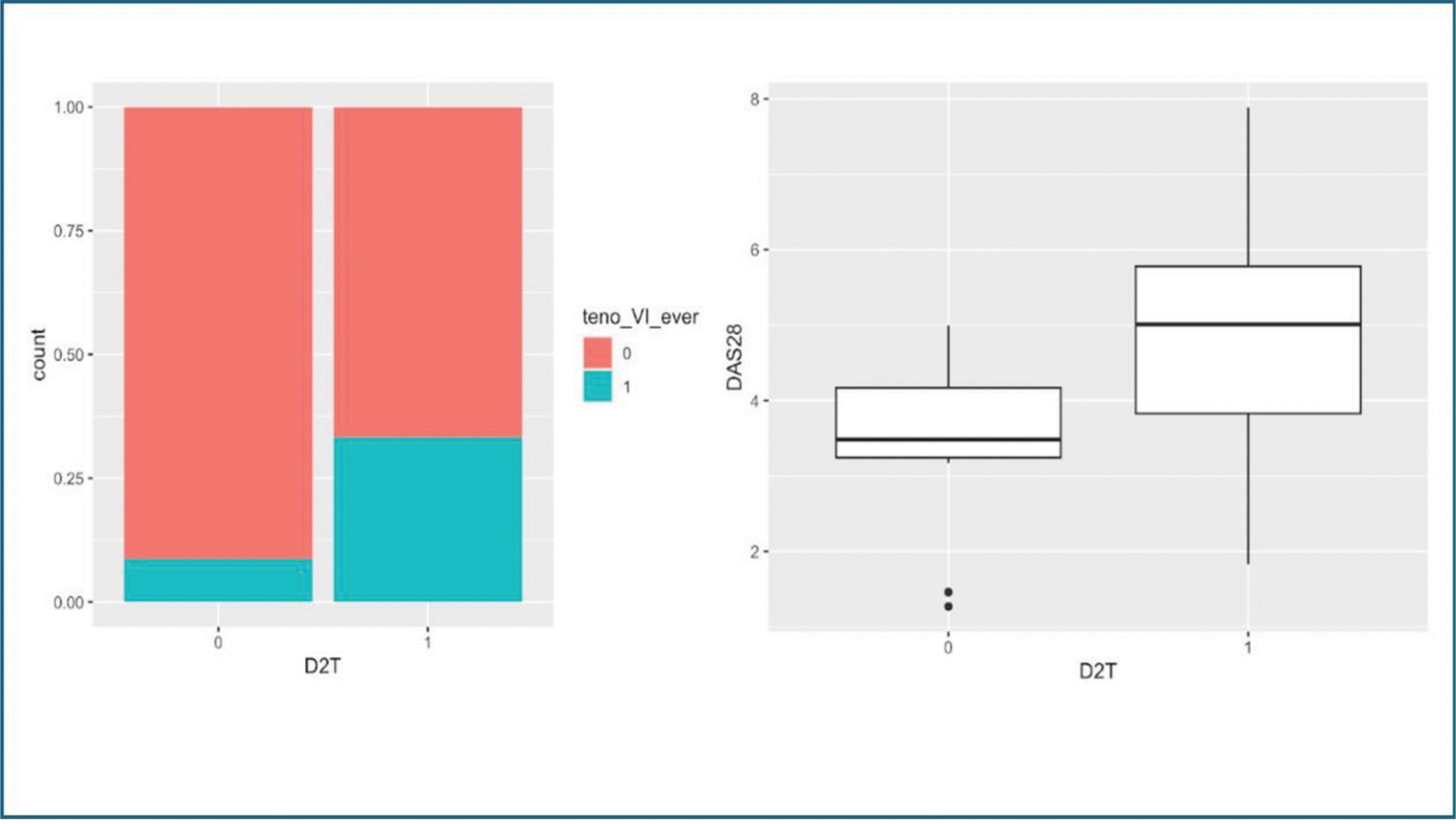
Results: One-hundred-twenty-four patients were included in the study (Table 1), with a median (±IQR) follow-up of 18.6 (11.98-25.22) years. Ninety-two (74%) patients fulfilled the EULAR criteria for D2TRA. Median age at diagnosis was lower in D2T patients, yet not reaching statistical significance (47 ±14.4 vs 55 ± 11.6, p=0.08). No significant difference was retrieved between D2TRA and non-D2TRA groups regarding cardiovascular diseases, diabetes, hypertension, prevalence of ILD and dysmetabolic comorbidities. Of the 124 patients, 56 underwent an US assessment before the administration of any b/tsDMARDs. Among them, 33 further progressed to be D2T. At the time of index US, patients who would later become D2TRA had higher DAS28 scores (4.4 vs 3.4, p=0.008). Thirty-one D2T (34%) and 21 non-D2T (65%) patients had US detectable synovitis. There was no statistically significant difference in the patterns of joints involvement neither in the number of inflamed joints per individual. In comparison to non-D2TRA patients, progressors to D2TRA often exhibited more extensive and severe synovitis with higher numbers of overall GS and PD values, yet not reaching statistical significance (total GS score 7.56 vs 9.42, p=0.32; total PD score 6.42 vs 8.36, p=0.32; total GS+PD score 17.9 vs 14.0, p=0.23). Tenosynovitis was observed in 20 progressors to D2T (21.7%) and 13 nD2T (41.9%) patients, respectively (p=0.97). In D2T group, patients with tenosynovitis displayed a higher mean DAS28-CRP (4.49 ±1.31 vs. 3.75± 1.08, p =0.023). Tenosynovitis of the VI compartment was more frequent in patients who would later become D2T (OR 5.1 [0.94-52.9], p =0.052). Erosions were found in 56 D2T (60.8%) and 17 nD2T (54.8%) (p=0.7) at baseline.
Conclusion: Patients that would later become D2T showed higher baseline values of disease activity. At index US, a higher prevalence of extensor carpi ulnaris involvement and a tendency towards higher inflammation scores was detected in further-to-be D2TRA patients. The presence of active tenosynovitis in D2T patients is associated with higher global disease activity scores, suggesting the importance of tendinous inflammatory component in the D2TRA phenotype.
REFERENCES: [1] Bellis E, Agugliaro F, Garulli C, et al. The role of musculoskeletal ultrasound in difficult-to-treat RA: Insights from a systematic literature review. Autoimmun Rev. 2025;24(1):103694. doi:10.1016/j.autrev.2024.103694.
[2] Nagy G, Roodenrijs NMT, Welsing PM, et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. 2021;80(1):31-35. doi:10.1136/annrheumdis-2020-217344.
[3] The 2017 EULAR standardised procedures for ultrasound imaging in rheumatology. Möller I, et al. Ann Rheum Dis. 2017.PMID: 28814430.
Tabel 1. demographic and clinical data of the cohorts.
Tenosynovitis of the VI compartment (left) and DAS28-CPR score (left) in D2T and non-D2T patients.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (