fetching data ... 
Background: Current knowledge considers enthesitis (inflammation of tendon and ligament insertions into bone) as the primary pathophysiological process in spondylarthritis (SpA), including both psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) [1]. However, enthesopathy and enthesitis can occur in otherwise healthy individuals and are associated with repeated mechanical overload, male sex, increasing age and high body mass index [2]. Musculoskeletal ultrasound (MSUS) can detect various inflammatory and structural lesions at the enthesis that can help to characterize SpA patients.
Objectives: We therefore aimed to determine which ultrasonographic lesions and which anatomical sites are best able to discriminate between SpA patients and healthy controls (HC).
Methods: We included patients with PsA and axSpA, followed within the Swiss Clinical Quality Management (SCQM) SpA databases from 5 Swiss hospital outpatient clinics, as well as HC. Following informed consent, participants completed a series of questionnaires and underwent a detailed clinical examination of both joints (66/68 joint count) and entheses, followed by a standardized MSUS examination protocol including 9 entheseal sites bilaterally (supraspinatus (Supra), lateral epicondyle (Lepi), medial epicondyle (Mepi), greater trochanter (Gtroch), Quadriceps (Quad), proximal patella (Pat), distal patella (Tib), Achilles (Achill), and plantar fascia (Plant)) by 6 rheumatologists experienced in MSUS from the SONAR group (
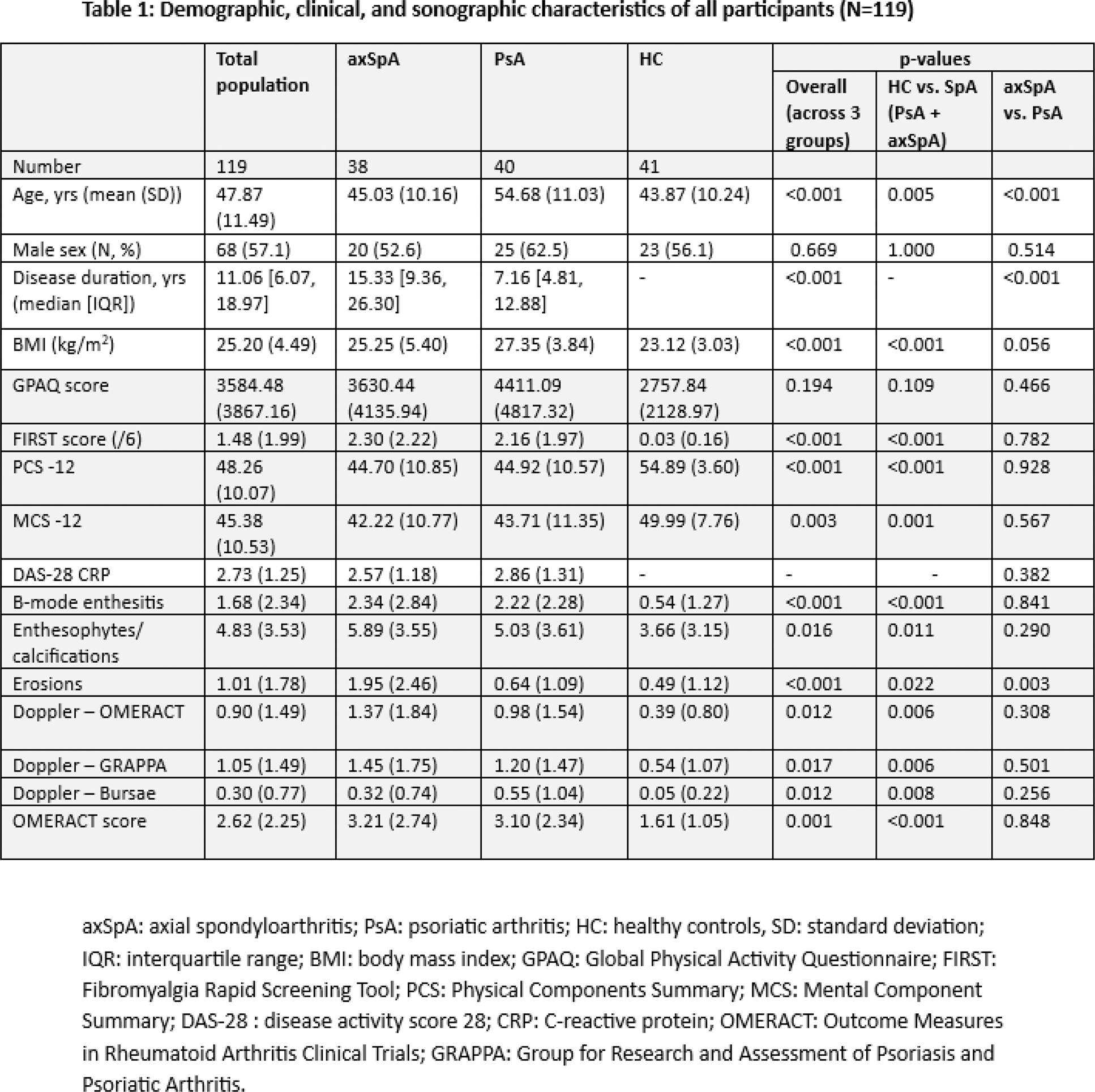
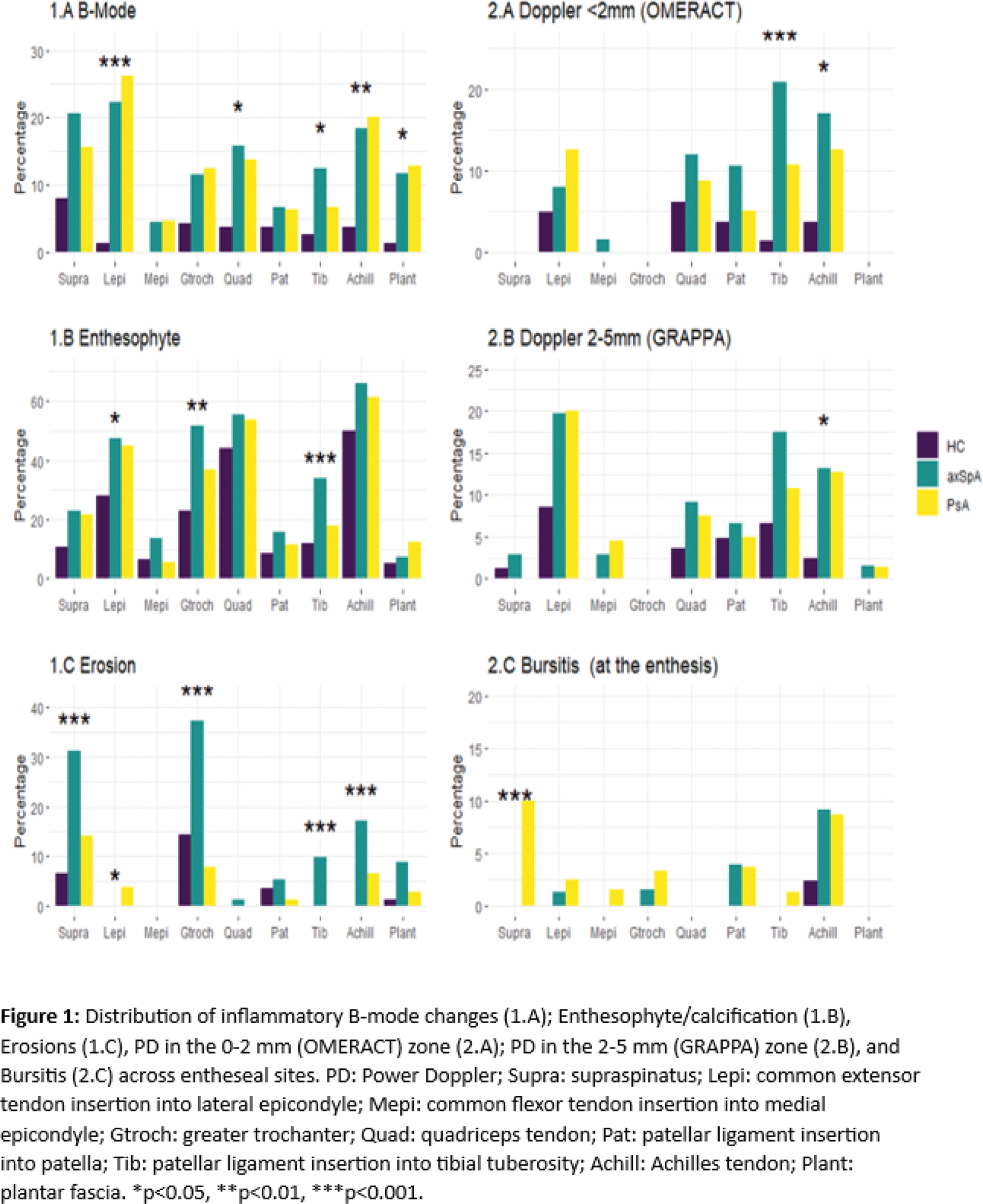
Results: Overall, 119 participants were included, including 40 PsA (mean age (SD), percentage male: 54.7±11.0, 62.5%), 38 axSpA (45.0±10.2, 52.6%) and 41 HC (43.9±10.2, 56.1%), with a total of 2142 entheses evaluated (Table 1). Most SpA patients (83.4%) had received biologic/targeted-synthetic DMARD. The PsA and axSpA groups showed no significant differences regarding erythrocyte sedimentation rate, C-reactive protein, Health Assessment Questionnaire, Bath Ankylosing Spondylitis Disease Activity Index, and tender/swollen joint disease activity scores. There were no significant differences between all three groups in terms of Global physical activity (GPAQ score). The prevalence of all elementary lesions was significantly higher in both forms of SpA compared to HC, with the exception of erosions. Across all entheses, erosions were significantly more common in axSpA (11.6%) vs. PsA (3.9%) (p<0.001), whilst only seen in 2.8% of HC. However, the differences between the three groups were dependent on the specific entheseal site and lesion (Figure 1). Interestingly, pronounced differences in inflammatory B-mode changes were only observed at certain sites (Lepi, Quad, Tib, Achill, and Plant). The prevalence of PD signal at the enthesis in both GRAPPA (6.2%) and OMERACT (5.4%) zones was similar and was significantly higher in both axSpA and PsA patients compared to HC, particularly at the Achilles and distal patella tendons. While enthesophyte/calcification was the most prevalent lesion across all groups, the only significant differences between groups were seen at 3 locations (Gtroch, Lepi, and Tib insertions). Furthermore, erosions were significantly more common in axSpA compared to PsA and HC, at the Supra, Tib, Gtroch, and Achill insertions (p < 0.001). Finally, bursitis was more prevalent in PsA patients, notably at the supraspinatus (p = 0.001).
Conclusion: Sonographic entheseal abnormalities such as enthesophytes/calcifications are commonly seen in HC and are therefore not specific to SpA. In addition to the recommended 2mm OMERACT zone, PD examination of the 5 mm zone should also be considered. To distinguish SpA patients from controls, any sonographic scoring system should account not only for the presence of particular lesions (structural and inflammatory) but also for the specific entheseal site affected. Our findings may assist with the development of a new composite US score that could improve the assessment of enthesitis in spondylarthritis.
REFERENCES: [1] A. D. Matteo
et al.
‘Relationship Between Ultrasound and Physical Examination in the Assessment of Enthesitis in Patients With Spondyloarthritis: Results From the DEUS Multicenter Study’,
Arthritis Rheumatol.
published online August 20, 2024. doi:
[2] A. L. Ribeiro and L. Eder, ‘From Psoriasis to Psoriatic Arthritis: Ultrasound Insights Connecting Psoriasis with Subclinical Musculoskeletal Inflammation and the Path to Psoriatic Arthritis’, Curr. Rheumatol. Rep. vol. 26, no. 7, pp. 235–247, Jul. 2024.
[3] P. V. Balint et al. ‘Reliability of a consensus-based ultrasound definition and scoring for enthesitis in spondyloarthritis and psoriatic arthritis: an OMERACT US initiative’, Ann. Rheum. Dis. vol. 77, no. 12, pp. 1730–1735, Dec. 2018.
Acknowledgements: Swiss Clinical Quality Management in Rheumatic Diseases (SCQM).
Disclosure of Interests: Gehad G. Elsehrawy: None declared , Delphine S Courvoisier: None declared , Erik Deman: None declared , Diana Dan for Eli Lilly, Novartis, UCB, GSK, Menarini, Viatris, Raphael Micheroli: None declared , Hans Ziswiler: None declared , Pascal Zufferey: None declared , Laure Brulhart Bletsas: None declared , Michael J. Nissen Abbvie, Amgen, Eli-Lilly, Janssen, Novartis, Pfizer and UCB (with payment to institution), Abbvie, Amgen, Eli-Lilly, Janssen, Novartis, Pfizer and UCB (with payment to institution), Novartis (with payment to institution).
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (