fetching data ... 
Background: Patients with systemic lupus erythematosus (SLE) typically accrue irreversible organ damage due to uncontrolled disease activity, disease flares, or long-term glucocorticoid treatment. Early diagnosis and treatment with advanced therapies are key to preventing organ damage accrual. Previous analyses of data from the 1-year pivotal TULIP trials (NCT02446912 and NCT02446899) and their 3-year long-term extension (TULIP LTE, NCT02794285) have demonstrated the efficacy of anifrolumab for controlling disease activity while simultaneously reducing glucocorticoid requirements. However, high attrition in the placebo arm of TULIP LTE due to re-randomization or loss to follow-up have prevented comprehensive analysis of the efficacy of anifrolumab for preventing damage accrual. Thus, the effect of anifrolumab on organ damage accrual rates remains unknown, particularly beyond the 4 years covered by the TULIP trials.
Objectives: The LASER study (Long-term Organ Damage: Anifrolumab versus Real-World Standard of Care in Adult Patients with Active Systemic Lupus Erythematosus, NCT06485674) aimed to evaluate the effectiveness of anifrolumab for preventing organ damage up to 4 years and to extrapolate time to organ damage progression up to 10 years in adult patients with moderately to severely active SLE. The study used an external control arm of patients who received real-world standard of care (RW SOC) from the University of Toronto Lupus Clinic (UTLC).
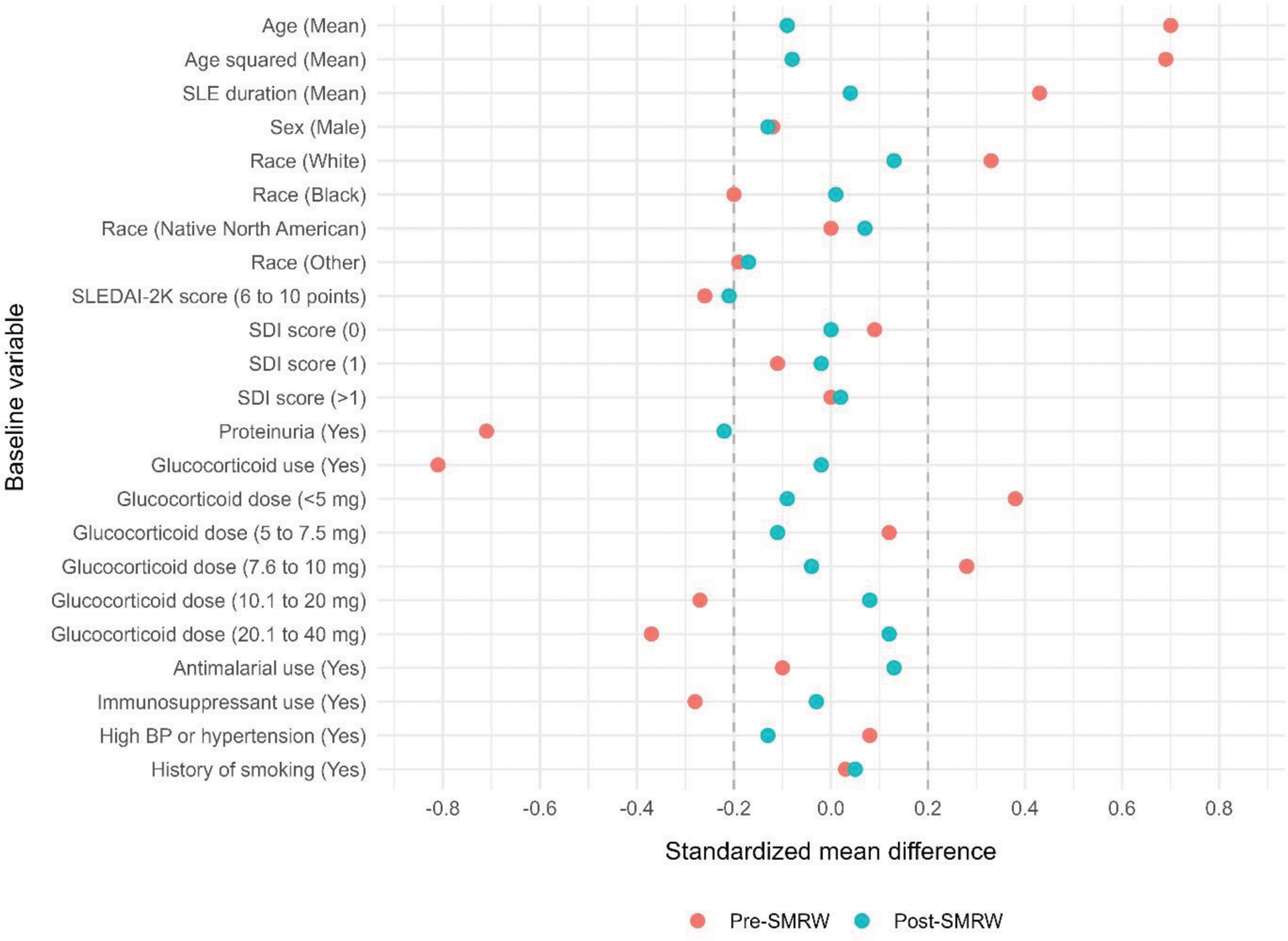
Methods: Patients who initiated 300mg anifrolumab in TULIP-1 or -2 were included in the anifrolumab arm; key eligibility criteria were applied to the UTLC to create the RW SOC arm. Propensity score (PS) and censoring weights were used to account for differences in baseline patient characteristics and losses to follow-up, respectively. 14 known predictors of organ damage were included in the PS models (Figure 1), and predictors which remained imbalanced following PS weighting were included in outcome models. Organ damage was measured using the Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI) score. Using data observed across 4 years of follow-up in TULIP, change in SDI score from baseline was estimated using weighted linear regression and time to first SDI score increase was estimated using Cox regression. Time to first SDI score increase within 10 years was then estimated using 7 separate parametric survival models fitted to data up to 4 years and extrapolated between 4 and 10 years; the best fitting parametric model (Royston-Parmar spline) was selected according to Akaike and Bayes information criteria values.
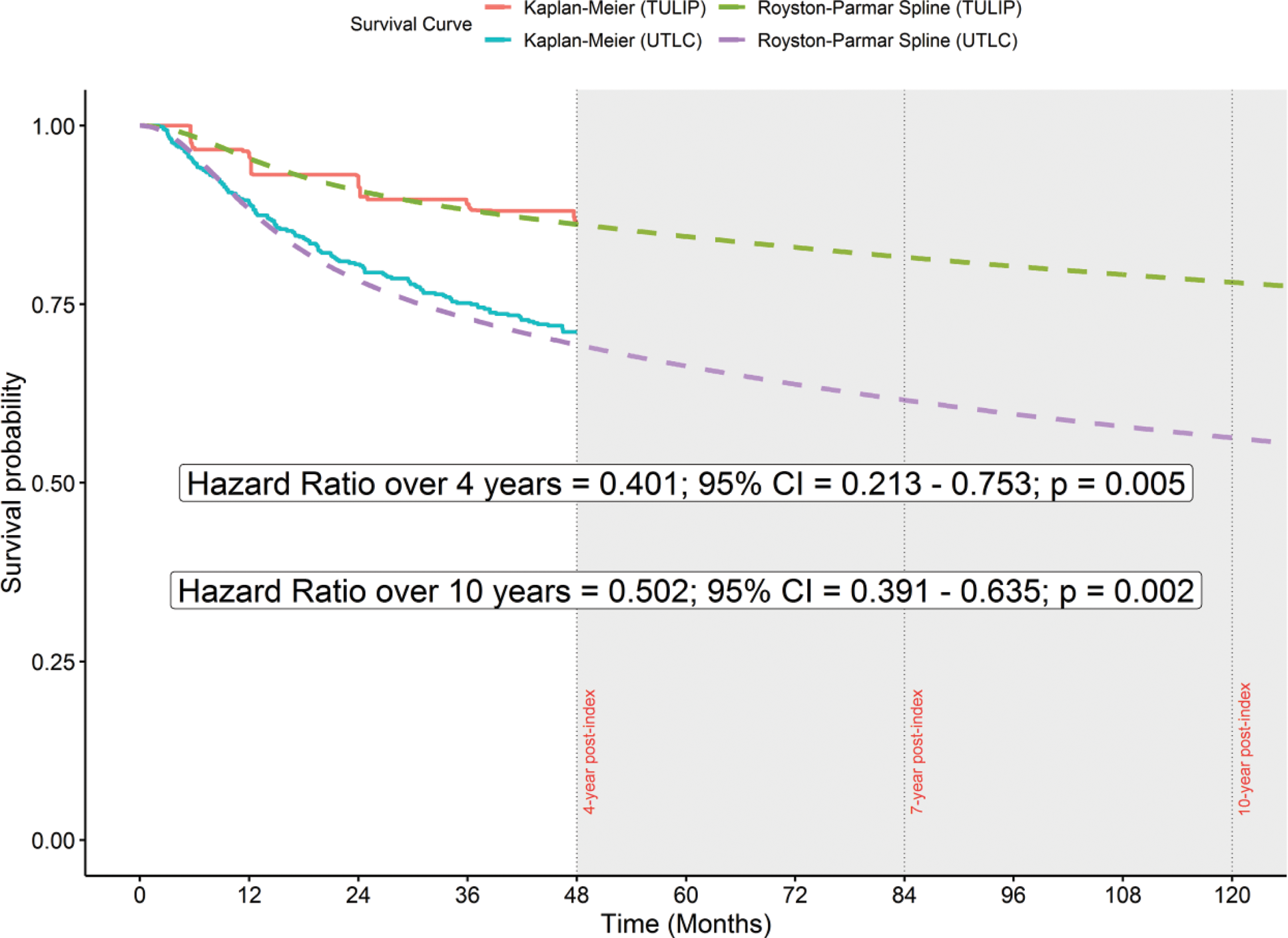
Results: 354 patients were included in the anifrolumab arm, and 561 patients were included in the RW SOC arm. Following PS weighting, baseline patient characteristics were adequately balanced (Figure 1). After accounting for differences in loss to follow-up, patients in the anifrolumab arm accrued 0.416 fewer points of organ damage (95% CI: -0.582, -0.249; p < 0.001) after 4 years and were 59.9% less likely (HR: 0.401, 95% CI: 0.213, 0.753, p = 0.005) to experience an increase in organ damage within 4 years compared to patients in the RW SOC arm. Using a Royston-Parmar spline model to extrapolate between 4 and 10 years, patients in the anifrolumab arm were 49.8% less likely (HR: 0.502, 95% CI: 0.391, 0.635, p = 0.002) to experience an increase in organ damage within 10 years (Figure 2).
Conclusion: Patients who received anifrolumab in the TULIP trials had accumulated significantly less organ damage up to 4 years compared to patients who received RW SOC. These results were supported by novel extrapolation analyses, which suggested that anifrolumab users would accumulate less organ damage over 10 years. The results of this study therefore support the benefit of adding anifrolumab to SOC for preventing long-term organ damage in patients with moderately to severely active SLE.
Baseline covariate balance before and after propensity score weighting.
Note that standardized mean differences < 0.2 (absolute value) indicate good covariate balance. SLEDAI-2K score and proteinuria were included in outcome models to further improve balance.
Abbreviations: BP = blood pressure; SDI = Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index; SLE = systemic lupus erythematosus; SLEDAI-2K = Systemic Lupus Erythematosus Disease Activity Index 2000; SMRW = standardized mortality ratio weighting.
Weighted Kaplan-Meier curves for observed time to organ damage progression up to 4 years, with 10-year extrapolations overlaid.
Note that the hazard ratio over 4 years was estimated from observed data using a Cox regression model; the hazard ratio over 10 years was estimated via extrapolation using a Royston-Parmar spline model.
Abbreviations: CI = confidence interval; TULIP = Treatment of Uncontrolled Lupus via the Interferon Pathway; UTLC = University of Toronto Lupus Clinic.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: Zahi Touma Speaker - AstraZeneca; Novartis; UCB Biopharma, Consultant - UCB Biopharma; Merck KgaA; GSK; Sarkana Pharma Inc.; Roche, Grant/Research Support - GSK, Ian Bruce Speaker - AstraZeneca; Janssen; GSK; Novartis, Consultant - AstraZeneca; Janssen; GSK; Novartis; Takeda; BMS, Richard A. Furie Speaker - AstraZeneca; GSK, Consultant - GSK; AstraZeneca; Genentech; Biogen; BMS; Kyverna; Novartis; Merck; EMD Serono; Ventas, Grant/Research Support - GSK; AstraZeneca; Genentech; Biogen; BMS; Kyverna; Novartis, Eric Morand Speaker - AstraZeneca; EMD Serono; Roche, Shares/Stock - Dragonfly, Consultant - AstraZeneca; Biogen; BMS; EMD Serono; Takeda; GSK; Novartis; Dragonfly; Alpine, Grant/Research support - Abbvie; AstraZeneca; Biogen; BMS; EMD Serono; Eli Lilly; Janssen; Takeda; UCB; GSK; Novartis; Roche, Raj Tummala Shares/Stock - AstraZeneca, Former Employment - AstraZeneca, Shelly Chandran Shares/Stock - AstraZeneca, Current Employee - AstraZeneca Canada, Gabriel Abreu Current Employee - AstraZeneca, Jacob Knagenhjelm Shares/Stock - AstraZeneca (indirect ownership through a mutual fund), Current Employee - AstraZeneca, Kellyn Arnold Current Employee - IQVIA, Tarana Mehdikhanova: None declared. Zheyuan Yang Current Employee - IQVIA, Hopin Lee Currently Employee - IQVIA, Danuta Kielar Shares/Stock - AstraZeneca, Current Employee - AstraZeneca, Miina Waratani Shares/Stock - AstraZeneca UK, Current Employee - AstraZeneca UK.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (