fetching data ... 
Background: Gout and hyperuricaemia are associated with various comorbidities, increased mortality and reduced quality of life. Gout care remains suboptimum worldwide with less than half of patients receiving urate-lowering therapy (ULT), usually without titration to achieve target serum uric acid(sUA) concentration levels. From our local data, only 21.9% and 33.9% of gout patients from primary care clinics and a tertiary rheumatology centre respectively achieved target sUA level of <360 µmol/L. In the UK, a randomised controlled trial (RCT) revealed more patients receiving nurse-led care had serum urate concentrations < 360 μmol/L at 2 years than those receiving usual care, whereas another RCT done in the US showed that a structured pharmacist-staffed program was more effective than usual care for achieving target sUA levels. These favourable outcomes, among others, prompted us to implement a structured gout management program in our local clinical setting.
Objectives: A pharmacist-, dietitian- and nurse-staffed One-stop Gout Clinic as part of a structured gout management program was implemented in our hospital since 2021. This retrospective observational study aims to highlight whether the structured program is more effective in achieving target sUA concentration levels and improving adherence to treatment compared to usual care in the General Clinic.
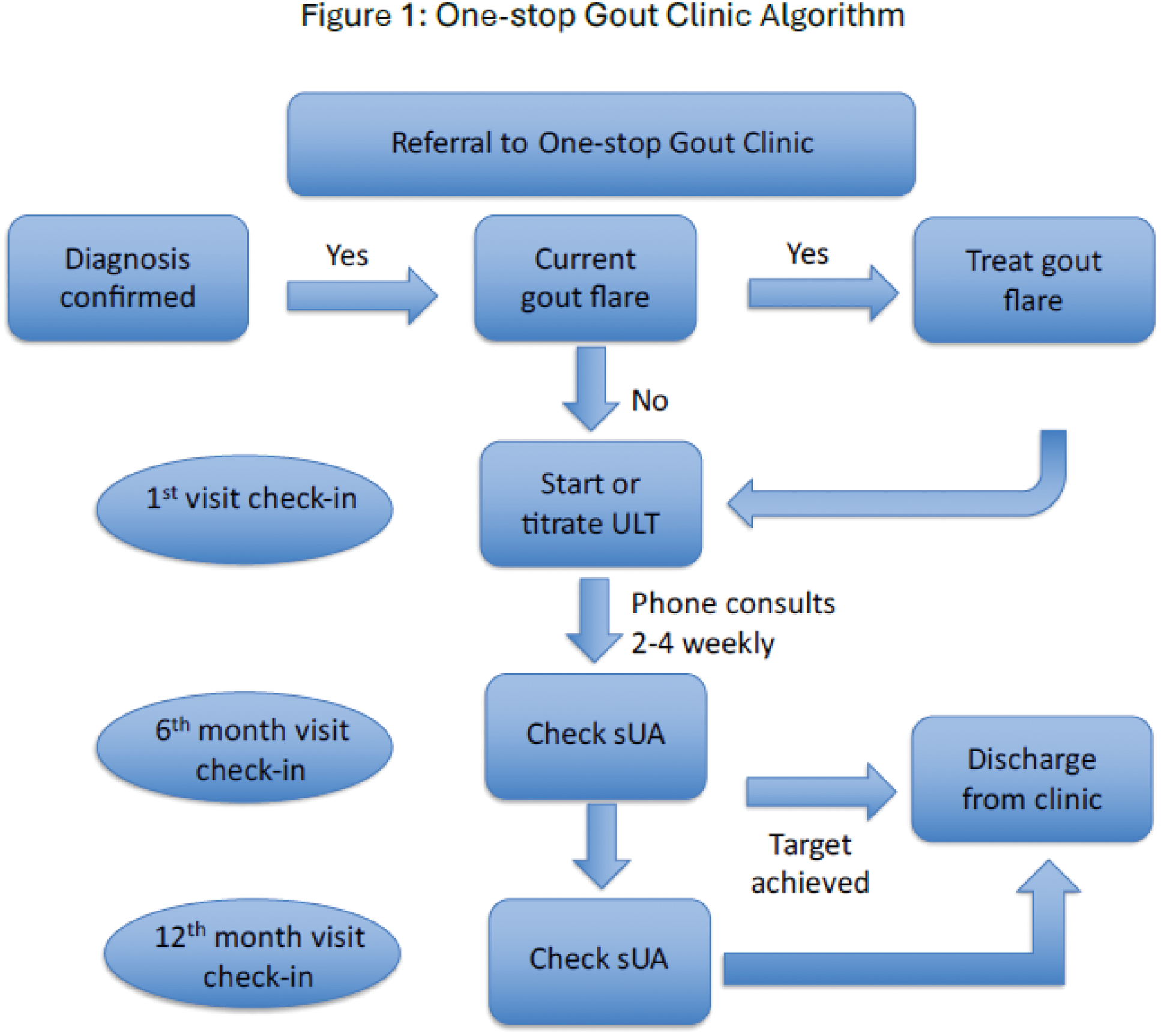
Methods: A retrospective review of the medical records of patients with established diagnosis of gout who were referred to the Rheumatology Clinic in a tertiary centre hospital within the period of 2 years from 2022 to 2023 were collected and analyzed using IBM SPSS Statistics Version 29.0.1. Patients who were seen at the One-stop Gout Clinic were reviewed by the Rheumatologist at the first clinic visit, followed by education and counselling by the assigned pharmacist, rheumatology specialist nurse and dietitian. Scheduled sUA level monitoring, teleconsultations and titration of ULT via a treat-to-target approach based on a drug titration protocol was done by the pharmacist and nurse in between clinic appointments, aiming to improve adherence and patient-centered outcomes. Patients were given subsequent clinic appointments at 6 months and 1 year. Following that, patients were discharged for follow-up and continuation of care at the primary care clinic (Figure 1).
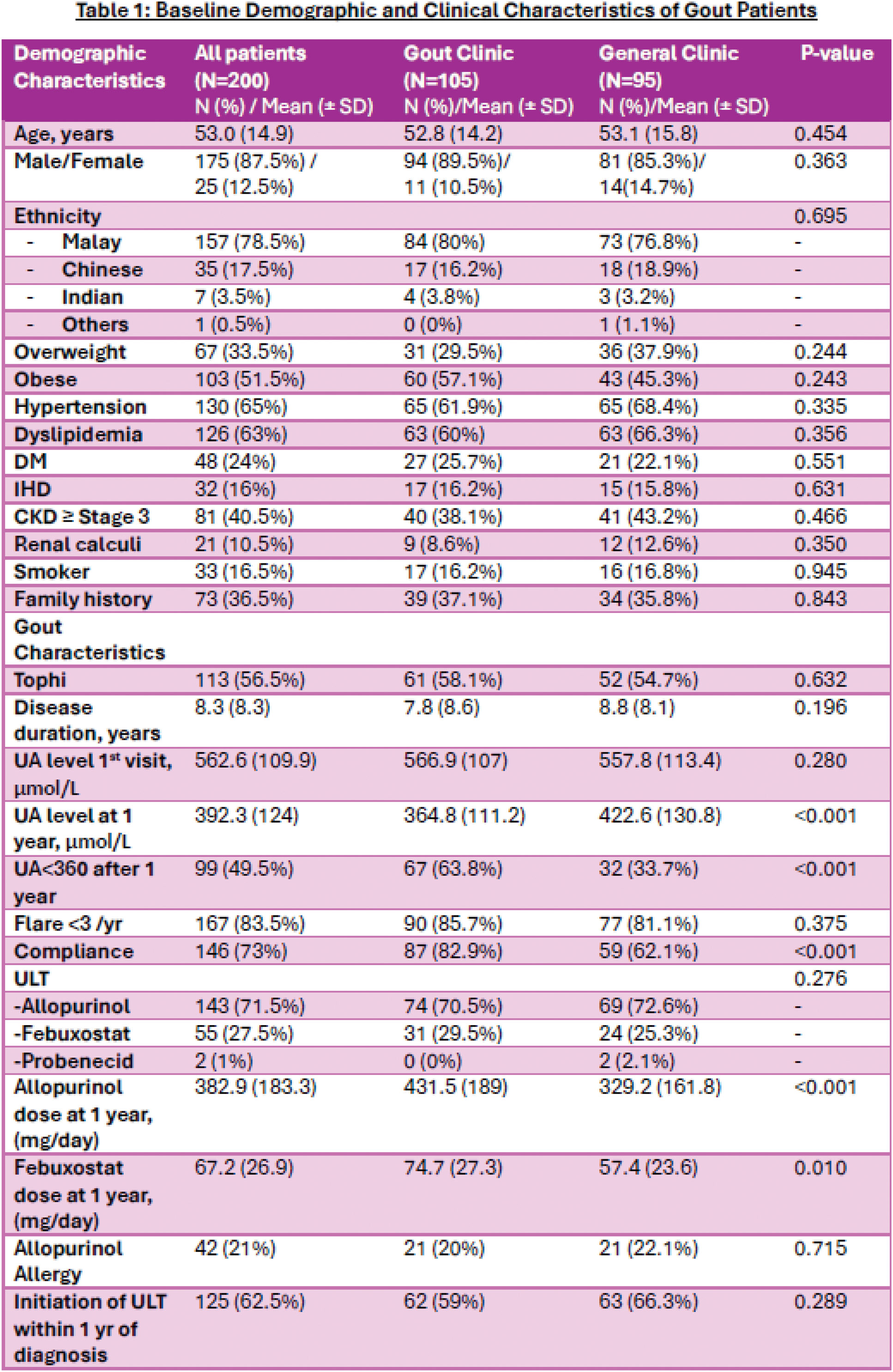
Results: There were 200 confirmed gout referrals received by the Rheumatology Department within the 2-year study duration, in which 105 patients were treated in the One-stop Gout clinic whereas 95 patients were treated in the General Clinic. Patients’ baseline demographic and clinical characteristics are listed in Table 1. Both groups had similar and comparable demographic and clinical characteristics. About half of the patients were obese (51.5%) and 40.5% of them had Chronic kidney disease Stage ≥3. Other comorbidities included Hypertension (65%), Dyslipidemia (63%), Diabetes mellitus (24%), Ischemic heart disease (16%), and renal calculi (10.5%). Slightly more than half of the patients (56.5%) had chronic tophaceous gout. The mean disease duration was 8.3 (± 8.3) years, and the mean sUA level at the first visit was 562.6 µmol/L (± 109.9). A substantial proportion of patients (62.5%) were initiated on ULT within the first year of diagnosis. There were 42 (21%) patients with history of allopurinol allergy. For the ULT used for gout treatment, majority of the patients (71.5%) were on Allopurinol, whereas 27.5% of patients were on Febuxostat and only 1% of the patients were on Probenecid. Notably, a significantly higher percentage of patients managed at the One-stop Gout Clinic achieved sUA of <360 µmol/L at 1 year as compared to patients seen at the General Clinic (63.8% vs 33.7%, p <0.001). The mean sUA level of patients in the One-stop Gout Clinic at 1 year follow-up was 364.8 µmol/L (± 111.2), which was significantly lower in comparison to the sUA of 422.6 µmol/L (± 130.8) in the General Clinic group (p<0.001). Allopurinol dose was significantly better optimized at 1 year in the One-stop Gout Clinic (431.5±189 mg vs 329.2±161.8 mg, p<0.001). Remarkably, patients from the One-stop Gout Clinic had better compliance (82.9% vs 62.1%, p<0.001) as compared to patients in the General Clinic. There was no statistically significant difference with regards to gout flare of less than 3 per year for both groups during the 1-year follow up period.
Conclusion: This study demonstrates the efficacy of the One-stop Gout Clinic in achieving target sUA level of <360 µmol/L within a year. Additionally, it showed improved patient compliance and optimization of ULT dosing compared to the General Clinic. The convenience of having allied health input in one setting together with scheduled drug titration schedules were the likely reasons for the success of this program. Furthermore, the study also provides insights into patient profiles and common comorbidities associated with gout. As the patients studied were referred to a tertiary referral center, the uric acid burden was higher as expected and associated with more complications, as reflected in the demographic data, with approximately half experiencing chronic tophaceous gout and extended disease duration. Notably, nearly half of these patients had CKD ≥ Stage 3, necessitating renal-adjusted doses of ULT and colchicine, alongside patient education on the cautious use of NSAIDs to prevent its complications and early referral to Nephrology team for CKD retardation. In conclusion, the One-stop Gout Clinic plays a vital role in the management of gout. Through a multidisciplinary collaboration among doctors, pharmacists, nurses, and dietitians, patients gain a deeper understanding of gout and its complications, which leads to improved compliance, better disease control and a reduction in complications.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (