fetching data ... 
Background: Keratoconus (KC) is a bilateral, progressive, non-inflammatory thinning and ectasia of the cornea. While traditionally considered non-inflammatory, recent studies have shown a positive association between KC and multiple immune-mediated diseases, suggesting that systemic inflammatory responses may influence its onset [Claessens et al, 2022].
Objectives: This study aimed to examine the association between prior exposure to autoimmune-rheumatic diseases (ARDs) and the development of KC using the Taiwan national health insurance research database (NHIRD).
Methods: A two-stage approach was employed. First, a nested matched case-control study was conducted to identify ARDs associated with KC. The ARDs of interest included Sjögren’s syndrome (SS), rheumatoid arthritis (RA), Graves’ disease (GA), systemic lupus erythematosus (SLE), and seronegative spondyloarthropathy (SpA). SpA included Crohn’s disease, ulcerative colitis, ankylosing spondylitis, and psoriasis/psoriasis arthritis [Snyder 2021]. Subsequently, a matched cohort study was performed to confirm these associations. For the case-control study, patients with newly diagnosed KC were identified from the NHIRD between 2008 and 2020. These calender years to identification KC was chosen to align with the significant increase in the use of corneal tomography in Taiwan since 2008, ensuring more accurate and reliable diagnosis of KC [Ng et al, 2024]. Patients with no prior history of eye clinic visits or corneal transplantation before their KC diagnosis were excluded. The index date was defined as the date of the first KC diagnosis. Age-, sex-, and index-date matched controls were randomly selected for each KC patient at a 4:1 ratio. Exposure to ARDs was assessed for periods of 1 to 10 years prior to the index date based on the date and relevant International Classification of Diseases (ICD) codes of the ARDs. For the cohort study, patients with the newly diagnosed ARDs, based on the findings of the case-control study, between 2008 and 2020 were identified. The index date was defined as the date of the first diagnosis of the respective ARD. Age-, sex-, and index-date matched controls were randomly selected for the ARD patient at a 2:1 ratio. The incidence of new KC was determined for periods of 1 to 10 years after the index date based on the date and relevant ICD codes of KC. Other covariates, including urbanization, occupation, and comorbidities (allergic rhinitis, asthma, collagen vascular disease, depression, diabetes mellitus, Down syndrome, hyperlipidemia, and sleep apnea), were also considered in the analysis [Lin et al, 2021]. Conditional logistic regression was used to estimate the adjusted odds ratio (OR) to assess the risk of KC associated with ARD. For the case-control study, the OR was estimated for periods of 1 to 10 years prior to the KC diagnosis date. For the cohort study, the OR was estimated for periods of 1 to 10 years following the ARD diagnosis date.
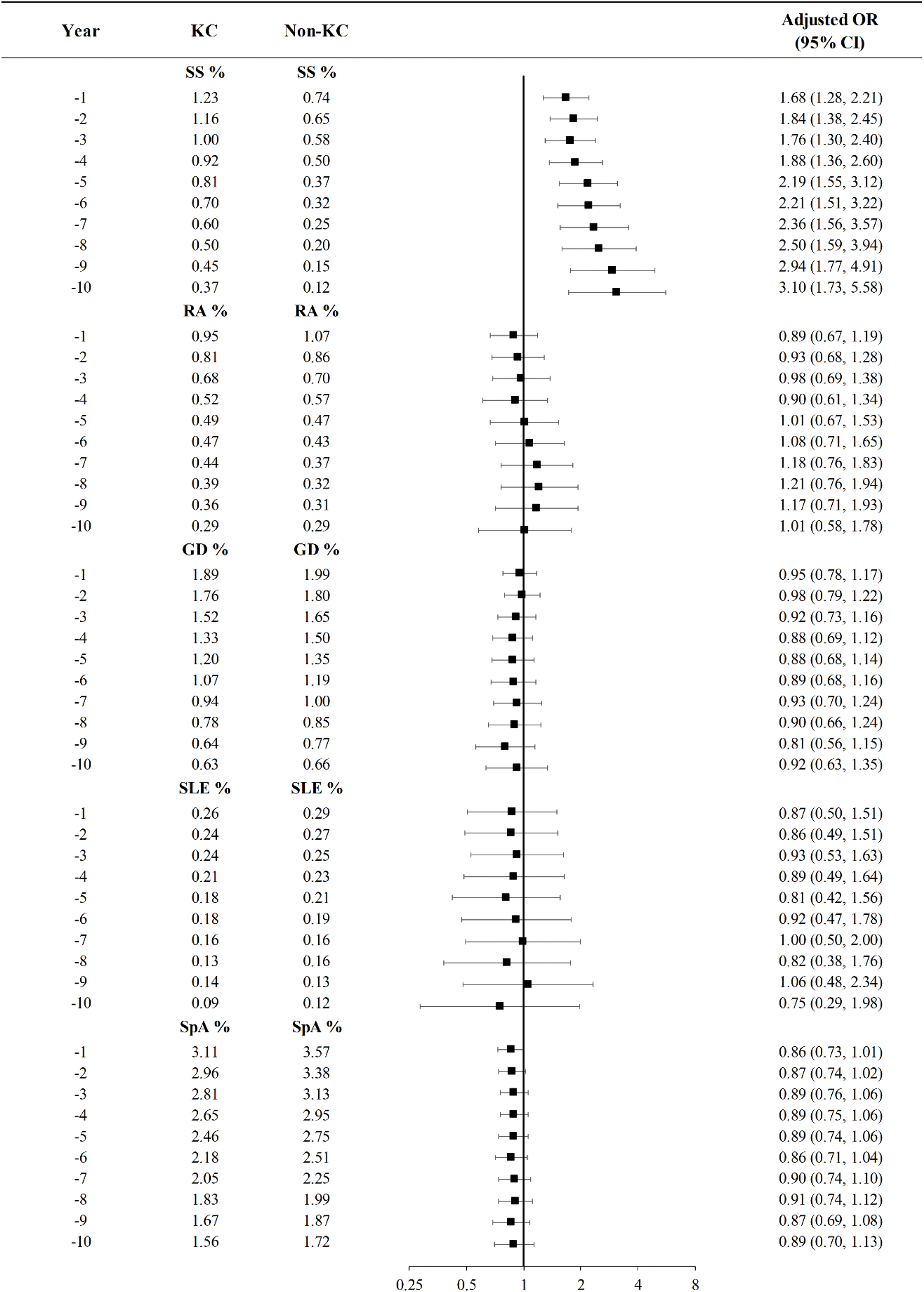
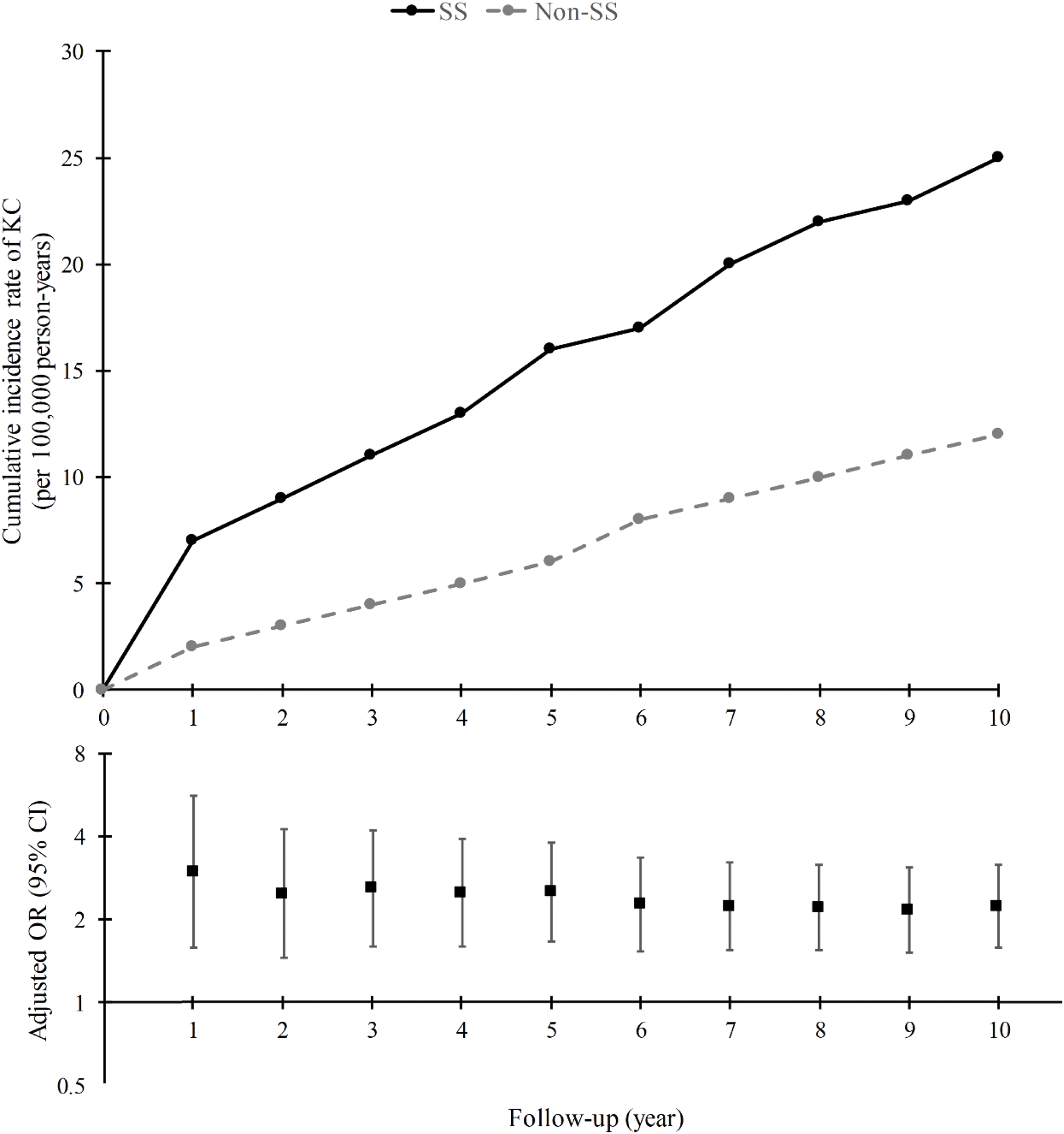
Results: The case-control study included 6183 new KC cases and 24732 matched controls. The mean age at first KC diagnosis was 27 years, and 59% of the cases were male. Sjögren’s syndrome (SS) was the only ARD significantly associated with KC (1.46% in the KC group vs. 0.84% in the control group), with an overall OR of 1.77 (95% CI: 1.95-3.25). This OR increased from 1.68 at 1 year to 3.10 at 10 years prior to the KC diagnosis date (Figure 1). The cohort study included 355382 new SS cases and 710764 matched controls. The mean age at first SS diagnosis was 52 years, and 74% of the cases were female. The 10-year cumulative incidence rate of KC (per 10,000 patients) was significantly higher in the SS cohort (1.9) compared to the non-SS cohort (0.9), with an overall OR of 2.05 (95% CI: 1.46-2.87). This OR decreased from 2.99 at 1 year to 2.23 at 10 years after the SS diagnosis date (Figure 2).
Presents a forest plot demonstrating the temporal relationship between autoimmune rheumatic diseases (ARDs) and keratoconus (KC) in the nested matched case-control study. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) are presented for exposure periods of 1 to 10 years preceding the diagnosis of keratoconus. These ARDs include Sjögren’s syndrome (SS), rheumatoid arthritis (RA), Graves’ disease (GD), systemic lupus erythematosus (SLE), and sero-negative spondyloarthropathy (SpA).
Illustrates the temporal trend of keratoconus (KC) risk following a diagnosis of Sjögren’s syndrome (SS) for the two cohorts. The upper panel displays the cumulative incidence rate of KC, while the lower panel presents a forest plot. The forest plot depicts adjusted odds ratios (ORs) and their 95% confidence intervals for exposure periods ranging from 1 to 10 years after the initial SS diagnosis.
Conclusion: This nationwide case-control and cohort study found a significant association between Sjögren’s syndrome (SS) and the development of keratoconus (KC). The overall OR between SS and KC was 1.77 in the case-control study and 2.05 in the cohort study.
REFERENCES: [1] Claessens JLJ, Godefrooij DA, Vink G, Frank LE, Wisse RPL. Nationwide epidemiological approach to identify associations between keratoconus and immune-mediated diseases. Br J Ophthalmol. 2022, 106(10):1350-1354.
[2] Lin KK, Lee JS, Hou CH, Chen WM, Hsiao CH, Chen YW,. & See LC. (2021). The sociodemographic and risk factors for keratoconus: nationwide matched case-control study in Taiwan, 1998-2015. Ame J Ophthalmol. 2021; 223: 140-148.
[3] Ng JM, Lin KK, Lee JS, Chen WM, Hou CH, & See LC. Incidence and prevalence of keratoconus in Taiwan during 2000–2018 and their association with the use of corneal topography and tomography. Eye, 2024; 38(4), 745-751.
[4] Snyder EA. Seronegative Spondyloarthropathies. In Clinical Foundations of Musculoskeletal Medicine: A Manual for Medical Students. Springer Nature Switzerland AG 2021;119-132.
Acknowledgements: grant from Chang Gung Memorial Hospital (CFRPG3N0061)
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (