fetching data ... 
Background: Anti-centromere antibodies (ACA) are generally considered protective against the development of interstitial lung disease (ILD) in systemic sclerosis (SSc). However, ILD can still occur and progress in ACA-positive patients.
Objectives: To analyze the prevalence, clinical characteristics, risk of ILD progression, and prognosis of ILD-SSc ACA-positive patients.
Methods: We conducted a multicenter retrospective observational study involving 277 patients who fulfilled the 2013 ACR/EULAR classification criteria for SSc. All patients had ILD confirmed by thoracic HRCT. A comparative analysis was performed across three groups: ACA-positive, ATA-positive, and ACA/ATA-negative patients.
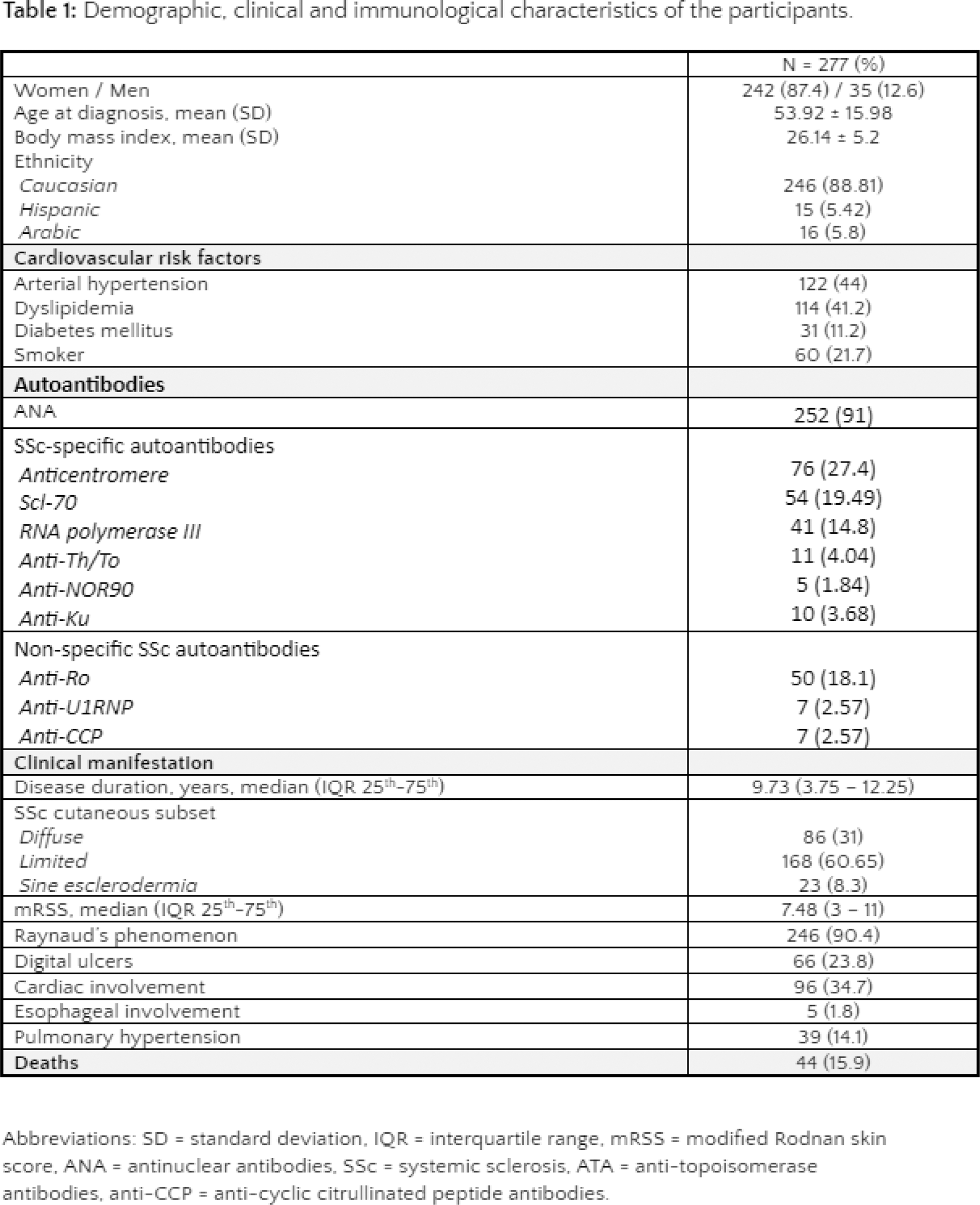
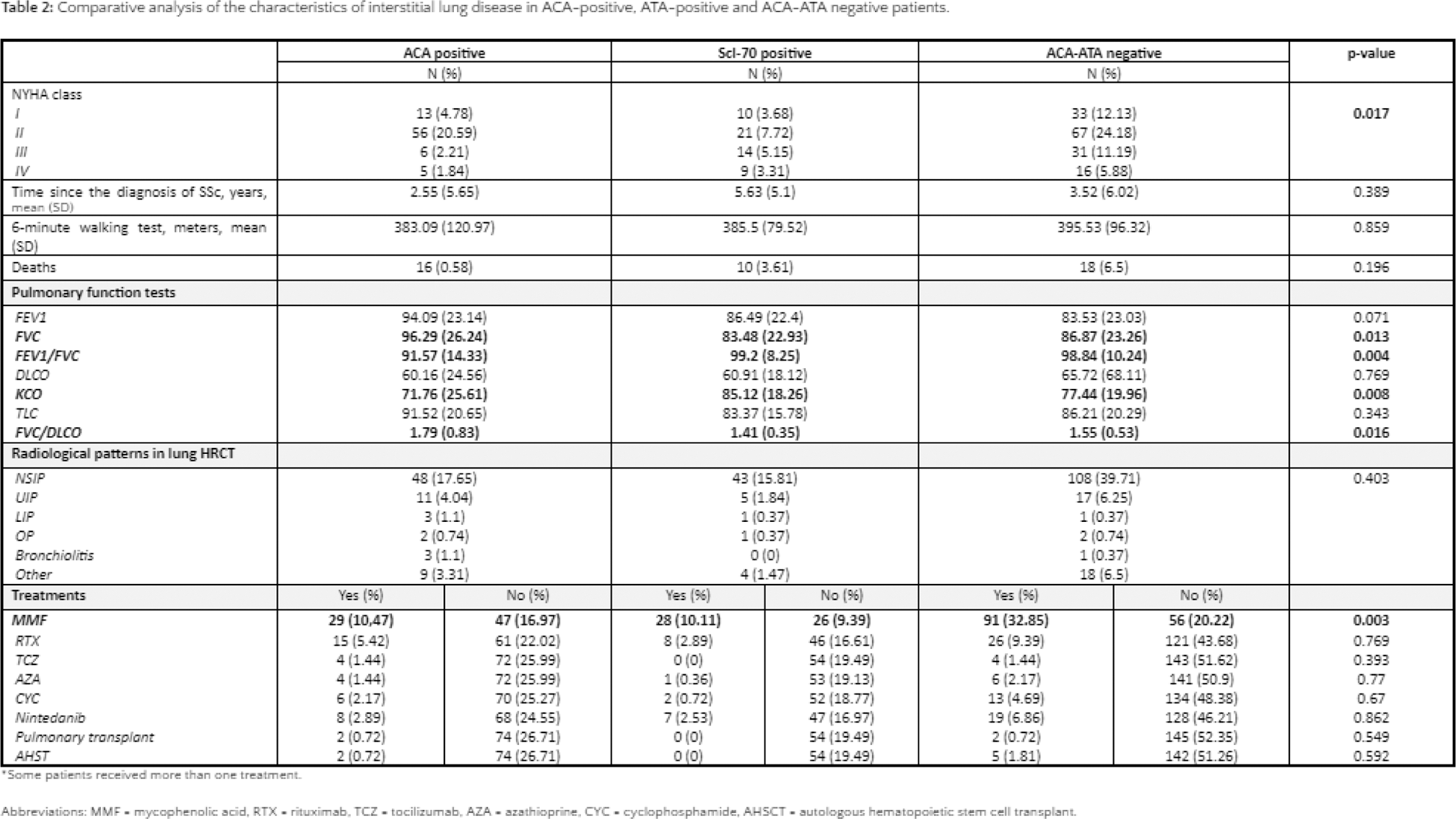
Results: The demographic and clinical characteristics of the study population are summarized in Table 1. Out of 277 patients, 76 (27.4%) were ACA-positive, 54 (19.5%) were ATA-positive, and 146 (53.1%) were ACA/ATA-negative. The comparative analysis of the three groups (see Table 2) indicates that ACA-positive patients exhibited a distinct ILD profile. Notably, these patients demonstrated better functional status, as reflected by their superior NYHA class (p=0.017), despite no significant differences in the 6-minute walking test (p=0.859) or mortality rates (p=0.196). The time from SSc onset to ILD diagnosis was comparable across groups (p=0.389), suggesting that ACA positivity does not significantly delay ILD onset. The predominant radiological pattern in all groups was NSIP, with no significant differences in other radiological patterns (p=0.403). Pulmonary function tests revealed that, at ILD diagnosis, ACA-positive patients had higher %FVC (p=0.013), FEV1/FVC ratio (p=0.004), %pDLCO (p=0.008), and FVC/DLCO ratio (p=0.016), indicating better preserved lung function compared to ATA-positive and ACA/ATA-negative patients. This likely explains the better clinical course observed in ACA-positive cases. Regarding treatment, ACA-positive patients were less frequently treated with mycophenolate mofetil (p=0.003), whereas the use of other therapies, including rituximab, cyclophosphamide, and nintedanib, showed no significant differences between groups. Notably, two ACA-positive patients (2.6%) required lung transplantation, and another two (2.6%) underwent autologous hematopoietic stem cell transplantation.
Conclusion: ACA-positive SSc-ILD represents a distinct phenotype, characterised by better preserved pulmonary function and less severe functional impairment compared to ATA-positive or ACA/ATA-negative ILD. However, ACA positivity does not ensure a benign disease course, as some patients may still experience severe progression, requiring advanced therapies, including lung or autologous stem cell transplantation.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (