fetching data ... 
Background: Subclinical GCA in PMR has been recently recognised as part of the GCA-PMR Spectrum of Disease [1]. Currently, vascular ultrasound is the only reliable method of identifying subclinical vascular inflammation in PMR patients [2]. So far, a simple biomarker for detecting concomitant arterial inflammation in PMR patients is lacking.
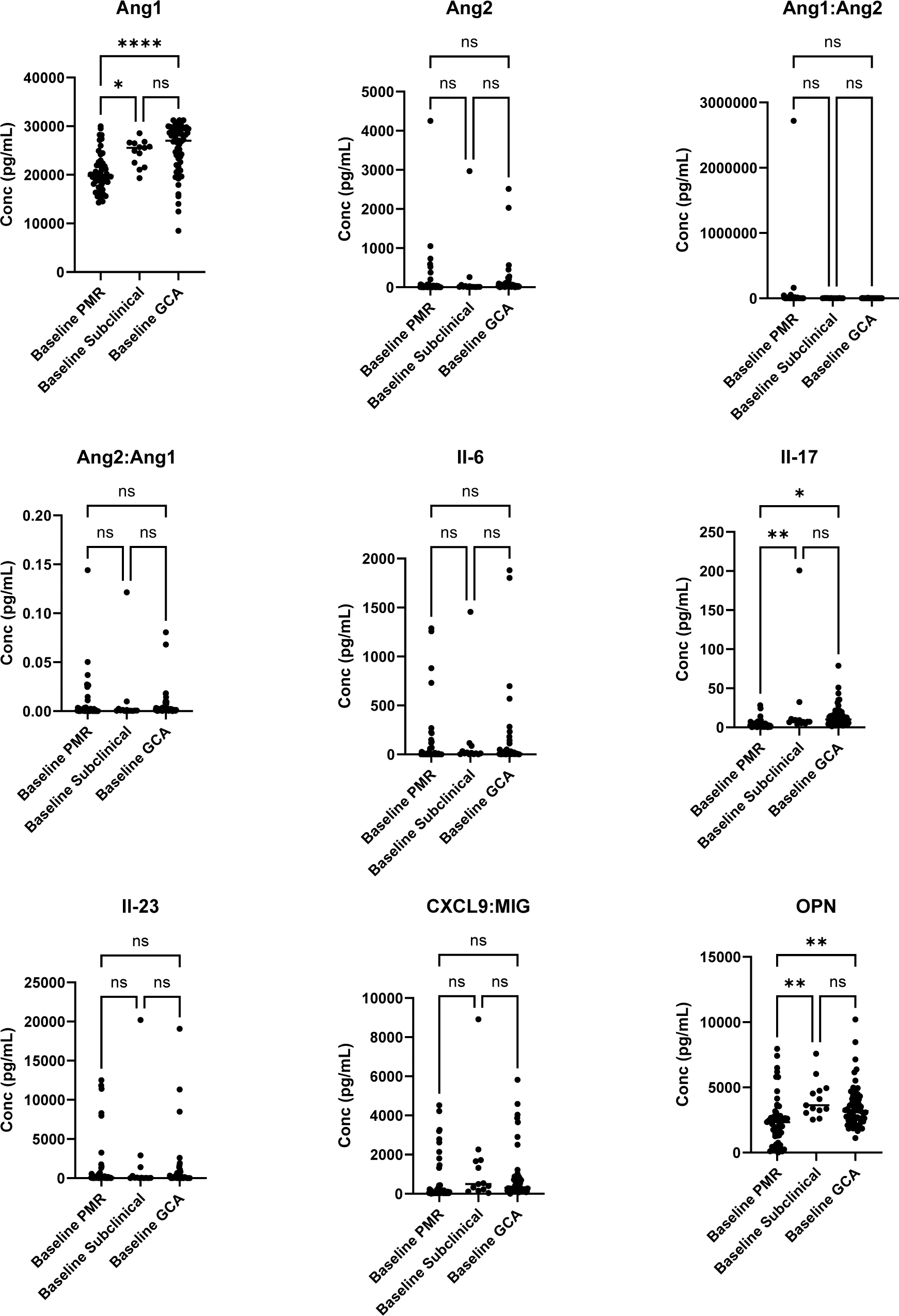
Objectives: The objective of this study was to investigate the diagnostic value of angiopoietin-1, angiopoietin-2, interleukin-6, interleukin-17A, interleukin-23, CXCL9, and osteopontin in subclinical GCA in PMR.
Methods: Fast-track GCA and PMR clinics were established at Tallaght University Hospital, Dublin and St James Hospital, Dublin to establish a multicentre prospective longitudinal study. Full ethical approval was awarded from the Joint Research Ethics Committee of TUH and SJH. Patients were prospectively recruited between July 2022 and July 2023; all gave written consent. Blood samples were collected from 53 PMR patients, 13 subclinical GCA in PMR patients, and 59 GCA patients. Samples were stored at -80 degrees and went through one freeze-thaw cycle. Serum levels of selected biomarkers were measured using the BioTechne ELISA screening assay kits following the manufacturer protocol recommendations.
Results: Angiopoietin-1 was significantly elevated in subclinical GCA in PMR compared with PMR patient serum (24,547.27pg/ml± 2678.68 vs 20,481.41pg/ml ±3865.11; p<0.001). ROC analysis showed the area under the curve to be 0.801 and a cut-off of 21,408pg/ml produced a sensitivity of 84.6% and a specificity of 70% for differentiating subclinical GCA in PMR from pure PMR. Baseline IL-17 levels were significantly elevated in subclinical GCA in PMR versus PMR (24pg/ml vs 3.9pg/ml; p<0.001). Osteopontin was significantly more elevated in subclinical GCA in PMR than pure PMR (4134.24pg/ml± 1441.35 vs 2446.54pg/ml ± 1879.13; p<0.01). Baseline levels of il-6, il-23, CXCL9, and angiopoietin 2 did not differentiate between PMR and subclinical GCA in PMR. Furthermore, there was no significant difference in baseline levels of all biomarkers between GCA and subclinical GCA.
Conclusion: Subclinical GCA in PMR has a biomarker signature that more closely resembles GCA than PMR. Baseline levels of angiopoietin-1, il-17, and osteopontin may help identify PMR patients with vascular inflammation. Angiopoietin-1 has the best sensitivity (84.6%) and specificity (70%) for identifying subclinical GCA in PMR patients. This may be a useful screening tool to identify PMR patients that would benefit from vascular ultrasound.
REFERENCES: [1] Tomelleri, A, et al., Disease stratification in GCA and PMR: state of the art and future perspectives. Nat Rev Rheumatol, 2023. 19 (7): p. 446-459.
[2] De Miguel, E, et al., Prevalence and characteristics of subclinical giant cell arteritis in polymyalgia rheumatica. Rheumatology, 2023. 63 (1): p. 158-164.
Table 1. Biomarker levels in subclinical GCA in PMR, GCA, and PMR.
Acknowledgements: Meath Foundation at Tallaght Hospital.
Disclosure of Interests: Sharon Cowley Novartis, Thomas Butler: None declared, Patricia Harkins Janssen Novartis, Colm Kirby: None declared, Danielle Molloy: None declared, Richard Conway Janssen Novartis, David Kane Novartis.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (