fetching data ... 
Background: Combination therapy with biologic/targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) and methotrexate (MTX) has been shown to be highly effective in controlling disease activity in rheumatoid arthritis (RA) patients. Given the chronic nature of RA treatment, the current challenge is to optimize safety and cost-effectiveness while maintaining treatment efficacy. Approximately half of RA patients treated with MTX reportedly have gastrointestinal symptoms or liver dysfunction, and some experience serious adverse events (SAEs). While discontinuation of concomitant MTX can reduce the adverse events (AEs) and increase safety in long-term treatment with b/tsDMARDs, it may cause a relapse in disease activity. Certolizumab pegol (CZP) is a PEGylated Fab’ fragment of a humanized anti-human tumour necrosis factor α monoclonal antibody. In general, PEGylation decreases immunogenicity and lengthens the circulating half-life of antibodies due to decreased clearance. CZP demonstrated clinical efficacy in monotherapy as well as with concomitant MTX in RA patients. These findings open up the possibility of MTX discontinuation in RA patients if disease control can be maintained.
Objectives: The present non-inferiority study was designed to compare the effect of discontinuing versus continuing MTX alongside CZP on maintaining low disease activity (LDA) in RA patients already stable on combination therapy.
Methods: The present study is a multicentre, open-label, randomized, controlled trial conducted in Japan. Participants were RA patients aged ≥20 years with sustained LDA (Clinical Disease Activity Index [CDAI] ≤10) for ≥12 weeks while receiving CZP + MTX. Patients were randomized 1:1 to the MTX continuation (CZP + MTX) and MTX discontinuation (CZP) groups. In the CZP group, the MTX dose was reduced by half at week 0, and discontinued at week 12 if LDA was maintained. In both treatment groups, CZP and conventional synthetic DMARDs other than MTX were continued at a stable dose throughout the course of the study. Rescue treatments were performed if the CDAI score was >10 or at the discretion of the investigator and/or upon patient request. The primary endpoint was the proportion of patients maintaining LDA without a flare at week 36 (24 weeks after MTX discontinuation). Disease flare was defined as a CDAI score >10 or intervention with rescue treatments for any reason. Non-inferiority is verified if the lower limit of the 90% confidence interval (CI) using normal approximation for the difference in the proportion of cases that maintained LDA at week 36 between the intervention group and control group exceeds the non-inferiority margin. Safety analysis included the incidence of AEs observed throughout the study period, and the Frequency Scale for Symptoms of Gastroesophageal reflux disease (FSSG) with a cut-off score of 8 for diagnosis of gastroesophageal reflux disease (GERD).
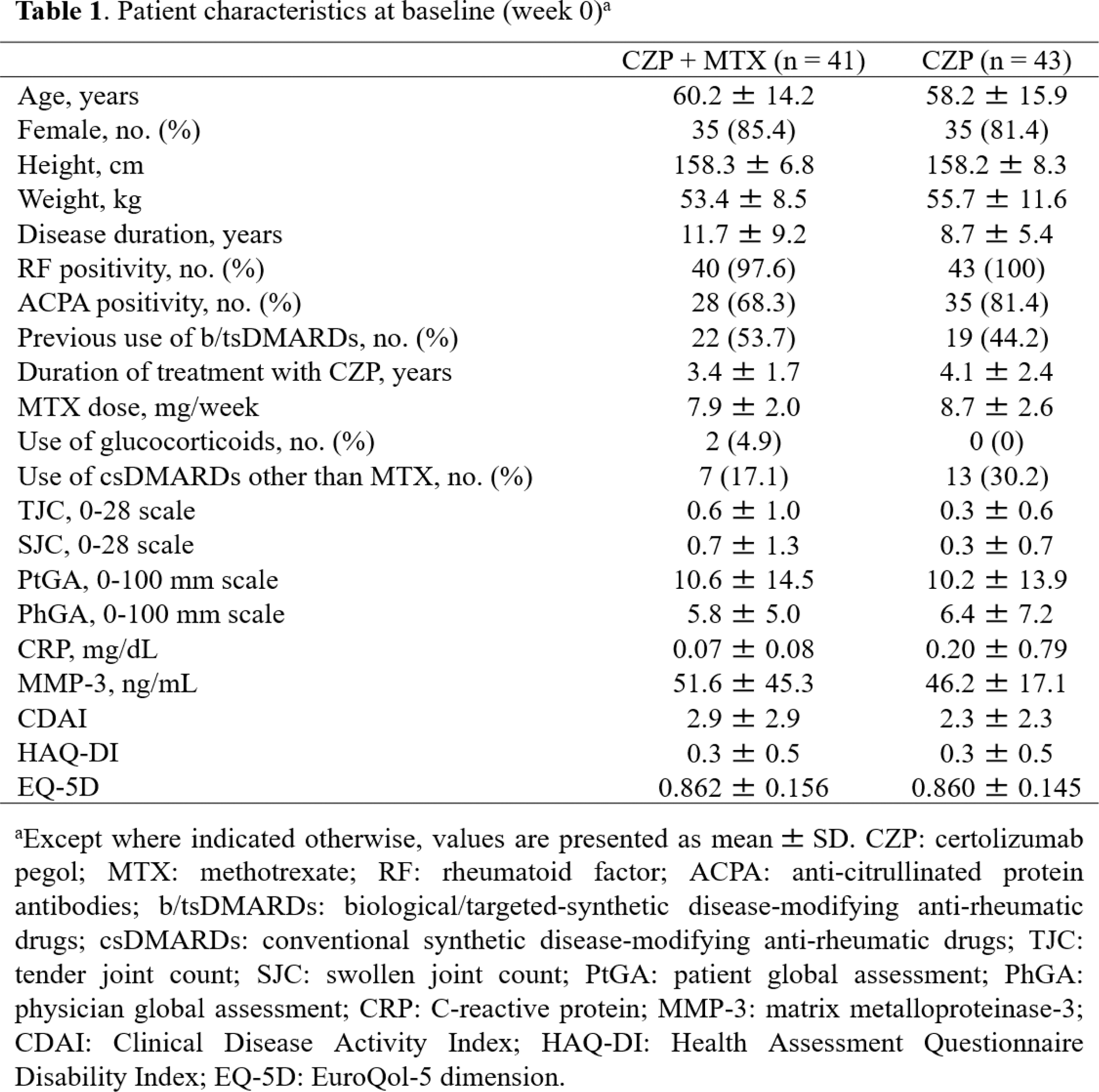
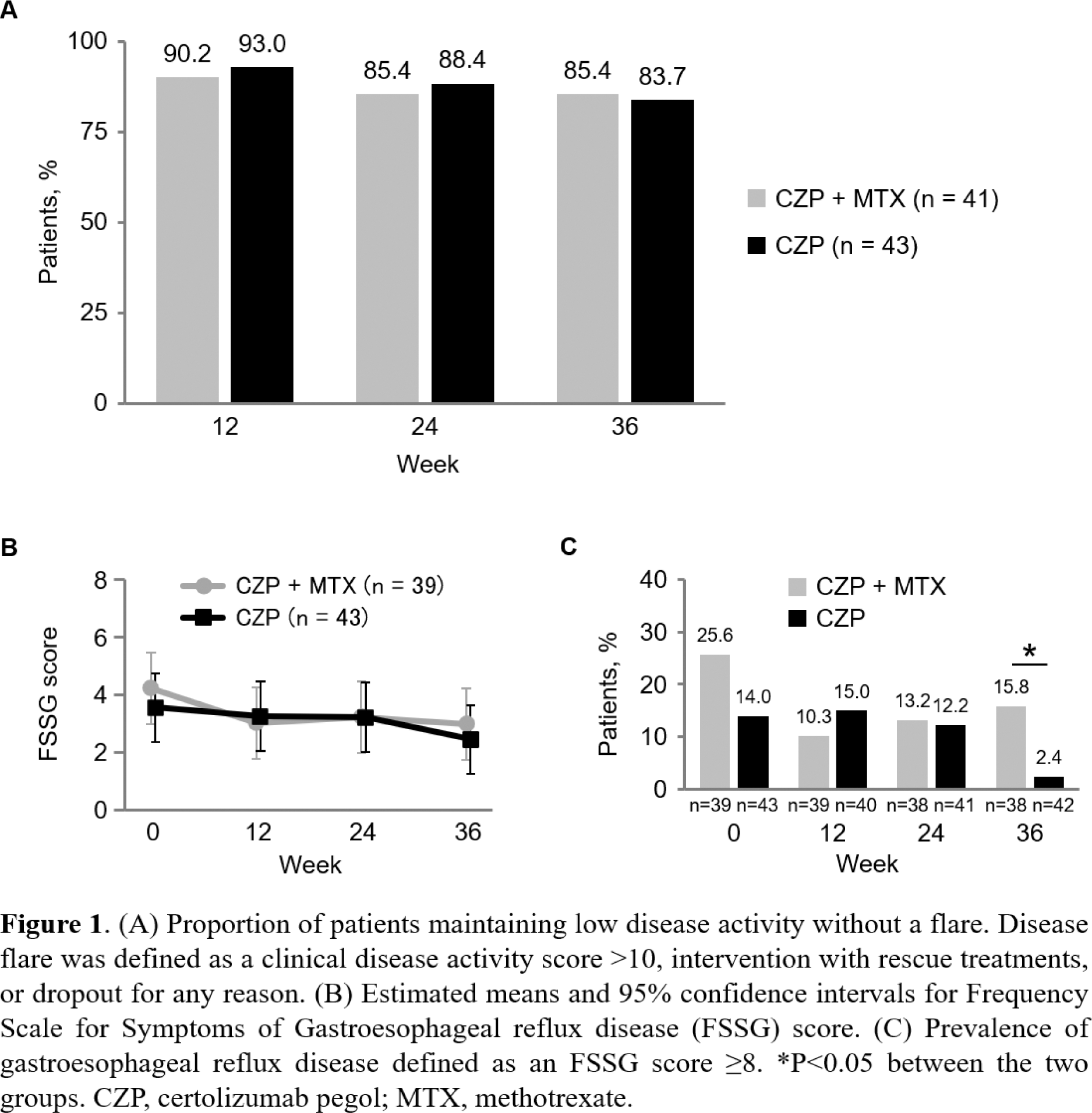
Results: All 84 enrolled patients were randomized to the CZP + MTX group (n = 41) and the CZP group (n = 43), and were included in the efficacy analysis. Table 1 shows the baseline (week 0) characteristics of patients included in the efficacy analyses. Demographic and clinical characteristics were balanced between the CZP + MTX and CZP groups. Proportions (90% CI) of patients who maintained LDA without a flare at week 36 were 85.4% (76.3 to 94.4%) in the CZP + MTX group and 83.7% (74.5 to 93.0%) in the CZP group (Figure 1A). The difference (90% CI) between the two groups was -1.6% (-14.6 to 11.3%), with the lower limit of the 90% CI exceeding the non-inferiority margin of -18%. The present study met its primary endpoint by demonstrating non-inferiority of the CZP group compared with the CZP + MTX group. There were no significant differences between the two groups at all time points in the estimated means and mean changes from baseline for the following parameters; CDAI, serum C-reactive protein and matrix metalloproteinase-3 levels, Health Assessment Questionnaire Disability Index, and EuroQol-5 dimension. AEs were broadly similar between the two groups during the period from week 0 to 36, and no SAEs were reported. There were no significant differences between the two groups in the estimated means and mean changes from baseline for FSSG score at all time points (Figure 1B). The prevalence of GERD was significantly lower in the CZP group than in the CZP + MTX group at week 36 (2.4% vs. 15.8%, P = 0.034), while there was no significant difference between the two groups at weeks 0, 12, and 24 (Figure 1C).
Conclusion: The results of the present study demonstrate that discontinuing MTX is non-inferior to continuing MTX in terms of maintenance of therapeutic effect in RA patients with sustained LDA treated with CZP + MTX.
REFERENCES: NIL.
Acknowledgements: We extend our deepest gratitude to Shinsuke Yasuda (Department of Rheumatology, Graduate School of Medical and Dental Sciences, Institute of Science Tokyo), Hisato Ishikawa (Department of Orthopaedic Surgery, Japanese Red Cross Aichi Medical Centre Nagoya Daiichi Hospital), Hiroaki Dobashi (Division of Haematology, Rheumatology and Respiratory Medicine, Department of Internal Medicine, Faculty of Medicine, Kagawa University), and Takako Hashimoto (Division of Rheumatology, Department of Internal Medicine, Fujita Health University School of Medicine) for their invaluable support and cooperation in conducting the present study.
Disclosure of Interests: Shuji Asai AbbVie, Asahi Kasei, Astellas, Ayumi, Chugai, Eisai, Eli Lilly, Taisho, UCB Japan, Astellas, UCB Japan, Toshihisa Kojima AbbVie, Astellas, Bristol-Myers Squibb, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly, Pfizer, Chugai, Taisho, Hajime Ishikawa: None declared, Nobumasa Miyake: None declared, Masanari Kodera: None declared, Hisanori Hasegawa AbbVie, Asahi Kasei, Astellas, AstraZeneca, Bristol-Myers Squibb, Eisai, GlaxoSmithKline, Nihon Pharmaceutical, Ono, Taisho, Japan Research Foundation Clinical Pharmacology, Yasumori Sobue: None declared, Yasuhide Kanayama Asahi Kasei, Astellas, Eisai, Eli Lilly, Hiromi Shimada: None declared, Yuji Hirano Astellas, UCB Japan, Toshihiko Hidaka AbbVie, Asahi Kasei, Bristol-Myers Squibb, Chugai, Eisai, Eli Lilly, Janssen, Pfizer, Takayoshi Fujibayashi: None declared, Takuya Matsumoto: None declared, Tomonori Kobayakawa: None declared, Hidekata Yasuoka AbbVie, Asahi Kasei, Astellas, Bayer, Boehringer Ingelheim, Chugai, Daiichi Sankyo, Eisai, Eli Lilly, Gilead, Kissei, Janssen, Nippon Shinyaku, Mitsubishi Tanabe, Novartis, Pfizer, Sanofi, Taisho, Takeda, Teijin, Viatris, Takefumi Kato: None declared, Masahiro Hanabayashi: None declared, Yuko Kaneko Astellas, Masahiro Tada: None declared, Koichi Murata Mitsubishi Tanabe, Pfizer, Ayumi, Mitsubishi Tanabe, UCB Japan, Kenta Misaki AbbVie, Asahi Kasei, Astellas, Boehringer Ingelheim, Chugai, Eisai, Eli Lilly, Gilead, Mitsubishi Tanabe, Mochida, Novartis, Ono, Pfizer, Taisho, Takeda, UCB Japan, Viatris, Masahiko Ando: None declared, Yachiyo Kuwatsuka: None declared, Mochihito Suzuki AbbVie, Asahi Kasei, Astellas, Chugai, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Mitsubishi Tanabe, Novartis, Pfizer, Sanofi, Taisho, Takeda, UCB Japan, Kenya Terabe AbbVie, Asahi Kasei, Astellas, Chugai, Eisai, Gilead, Mitsubishi Tanabe, Novo Nordisk, Pfizer, Sanofi, UCB Japan, AbbVie, Japan Rheumatism Foundation, Shiro Imagama: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (