fetching data ... 
Background: Virtually all patients with Eosinophilic Granulomatosis with Polyangitiis (EGPA) have asthma that develops years before vasculitis. Interestingly, the interplay between eosinophilic asthma (EA) and vasculitis is only partially understood. To date, a comparison between EGPA and EA to discriminate between these two conditions based on respiratory tract manifestations is lacking.
Objectives: This study was undertaken to investigate the association between respiratory manifestations and the risk of EGPA, as compared to EA.
Methods: Single-centre observational study in a referral center for vasculitis. Patients with EGPA comprising this cohort fulfilled the 2022 American College of Rheumatology (ACR)/ European Alliance of Associations for Rheumatology (EULAR) classification criteria for EGPA, while a diagnosis of EA was established according to the definition of the Global initiative for asthma (GINA) guidelines. Data from two retrospective cohorts, i.e. an EGPA cohort (collected from 1990 through 2022) and the eosinophilic asthma cohort (collected from 2001 to 2010) were updated and analysed. For each patient with EGPA, comparators with eosinophilic asthma were randomly selected from the eosinophilic asthma cohort and were matched for age (±5 years), sex, and years from asthma diagnosis to index date (i.e. the time between asthma diagnosis and the clinical assessment registered in the database). For EGPA, the index date (i.e. the date of the clinical assessment) was the date of EGPA diagnosis. Medical records of cases and comparators were reviewed for demographic and clinical data, including respiratory manifestations, laboratory parameters, pulmonary function measurements, and asthma treatments.
Results: Data had been collected for n=131 EGPA and n=350 for EA in the original databases. After removing those subjects with incomplete data and duplications, 97 EGPA patients were 1:1 matched for age, sex, and years from asthma diagnosis to index date with EA patients. Of the 97 EGPA patients, 50.5% were female, mean age was 52 (±13) years old, with 4 years (IQR 1, 15) between asthma diagnosis to index date. Myeloperoxidase-ANCA was positive at diagnosis in 35% of patients, and Five Factor Score was ≥1 at diagnosis in 94% of cases. Asthma was severe according to the ATS definition in 42.2% of subjects with EGPA and in 32.0% with EA (p=0.2953), chest X-ray abnormalities were reported in 68.0% of subjects with EGPA vs 51.6% with EA, and pulmonary infiltrates was reported in 62.9% vs 22.7% (p<0.0001), respectively. Nineteen (19.6%) subjects with EGPA had pleural effusion compared to none with EA (p<0.0001), and 16.5% with EGPA had gastrointestinal reflux vs 14.4% with EA (p=0.8429). Chronic rhinosinusitis was observed in 82.5% of subjects with EGPA vs 50.5% with EA (p<0.0001), with 45.7% vs 38.1% of subjects undergoing surgery for nasal polyps (p=0.3061), respectively. Mean (SD) BMI was 26.41 (5.31) for EGPA subjects vs 28.71 (5.59) for EA subjects (p=0.0056). Peripheral blood eosinophil (PBE) counts were significantly higher in EGPA subjects compared to EA subjects (6400cells/μL (IQR 3167, 12713) vs 320/μL (IQR 132, 610); p<0.0001), with 97.9% of EGPA subjects having PBE >10% and/or >1500/μL vs 13.4% of EA patients (p<0.0001). No difference in total IgE level was observed. 46.4% of EGPA subjects vs 91.2% of EA subjects (p<0.0001) were atopic (i.e. positive prick test and/or blood specific IgE for respiratory allergens), and 44.3% vs 13.4% had aspirin hypersensitivity (p<0.0001). Interestingly, no difference in the main pulmonary function test measurements was observed between cases and comparators (FEV1%, FEV1/FVC, reversibility%), however the diffusing lung capacity of CO was slightly lower in EGPA (DLCO, mean (SD), 86.2% (17.8) vs 94.0% (14.7), p=0.0121). 59.8% of EPGA subjects and 22.7% of EA subjects were receiving oral corticosteroids (OCS) at index date, while 75.0% of EGPA patients and 65.0% of EA patients were receiving inhaled corticosteroids (ICS), p=0.1578. Patients with rhinosinusitis, any chest X-ray abnormalities, and pulmonary infiltrates had significantly higher odds of having EGPA (OR (95% IC): 4.61 (2.39, 8.89); 2.00 (1.12, 3.59); 5.77 (3.08, 10.84), respectively), while patients with atopy had significantly higher odds of having EA (0.08 (0.03, 0.21)). Interestingly, severe asthma and surgery for nasal polyps were not associated with EGPA diagnosis (Figure 1).
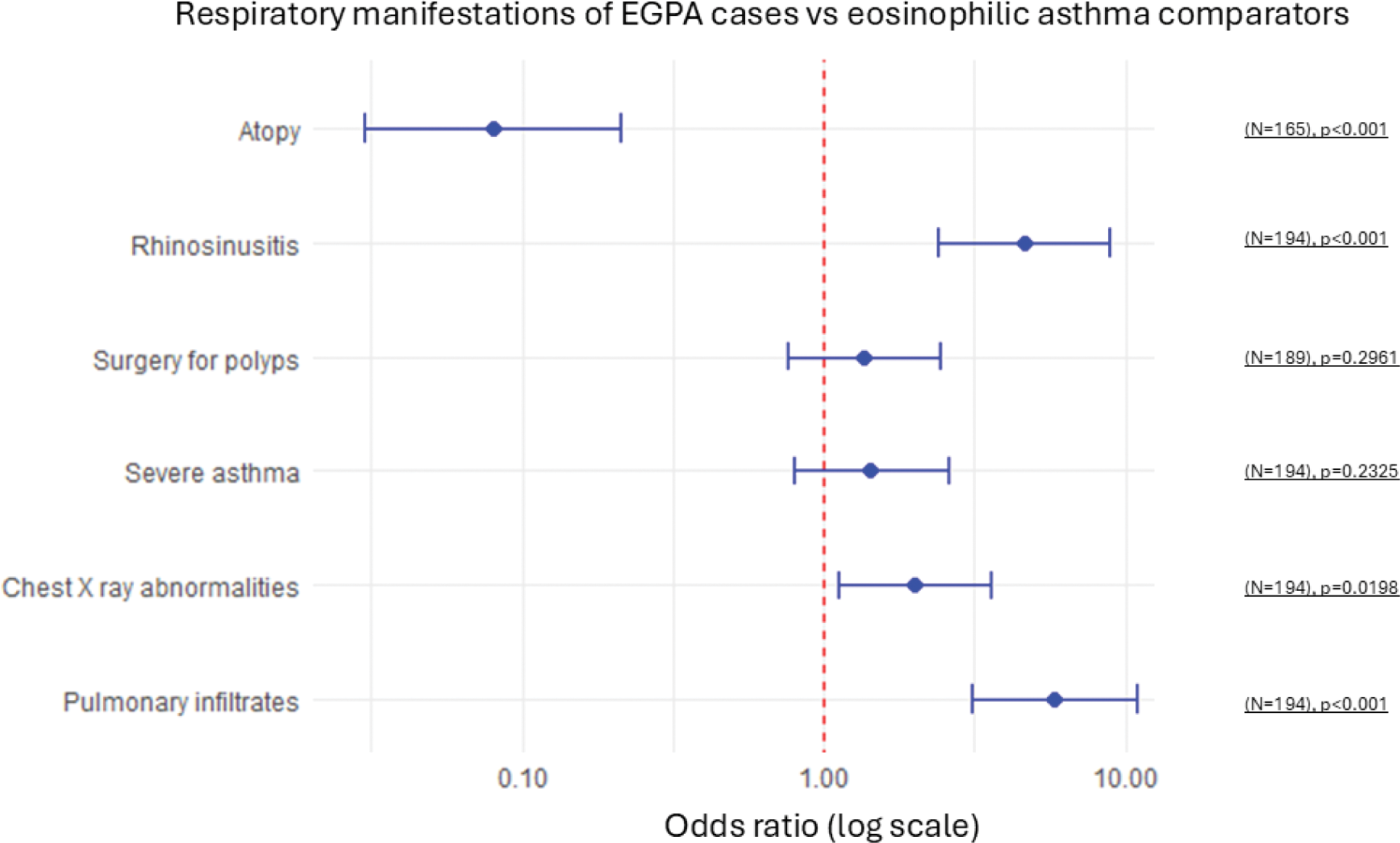
Conclusion: Compared to EA, EGPA patients at diagnosis have a different profile of respiratory manifestations, substantially higher levels of PBE, and higher proportion of patients using OCS. In this case-control study, those patients who had rhinosinusitis, any chest X-ray abnormalities, and pulmonary infiltrates, compared with those that did not, had significantly greater odds of having EGPA. Surprisingly, no significant odds were found for severe asthma and surgery for nasal polyps, challenging the common assumption that patients with severe asthma and/or rhinosinusitis may be at higher risk of developing EGPA.
REFERENCES: NIL.
Acknowledgements: NIL.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (