fetching data ... 
Background: Avascular necrosis (AVN) is a debilitating condition resulting from bone tissue death due to insufficient blood supply, commonly linked to corticosteroid (CS) use, alcohol consumption, trauma, and systemic diseases like rheumatologic conditions. AVN causes progressive joint destruction, severe pain, and reduced quality of life, often necessitating invasive interventions such as joint replacement. CS, essential in treating many inflammatory diseases, significantly increase AVN risk, correlating with both dose and duration. Additionally, diseases like systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and vasculitis independently elevate AVN risk through inflammation-induced vascular damage. Identifying high-risk patients enables tailored CS management, improving outcomes. However, data comparing AVN risk across rheumatologic diseases remain limited, underscoring the need for refined monitoring and risk stratification strategies.
Objectives: This retrospective study aims to evaluate the cumulative corticosteroid dose, time to AVN development, and disease-specific differences in AVN onset and frequency in patients with rheumatologic conditions to inform clinical decisions, reduce unnecessary healthcare costs, and improve patient outcomes through earlier recognition and tailored management.
Methods: This single-center, retrospective study included patients diagnosed with various rheumatic diseases who developed AVN following corticosteroid therapy. AVN was confirmed via imaging performed due to pain symptoms during routine outpatient visits (Figure 1). A control group was established, consisting of patients with the same diagnoses who had not developed AVN. Controls were matched in a 1:1 ratio based on age, gender, rheumatologic diagnosis, and cumulative corticosteroid dose. Data collected from patient records included demographic characteristics, underlying diagnoses, corticosteroid doses and durations, time to AVN diagnosis, imaging findings, and AVN-related treatments. The cumulative CS dose was calculated, and the time between corticosteroid initiation and AVN development was analyzed. Differences in AVN onset and frequency among rheumatologic diseases were also evaluated. CS dosing was categorized as follows: low dose: ≤7.5 mg/day of prednisolone (PRD), moderate dose: 7.5–30 mg/day of PRD, high dose: 30–100 mg/day of PRD, and pulse dose: >100 mg/day of PRD.
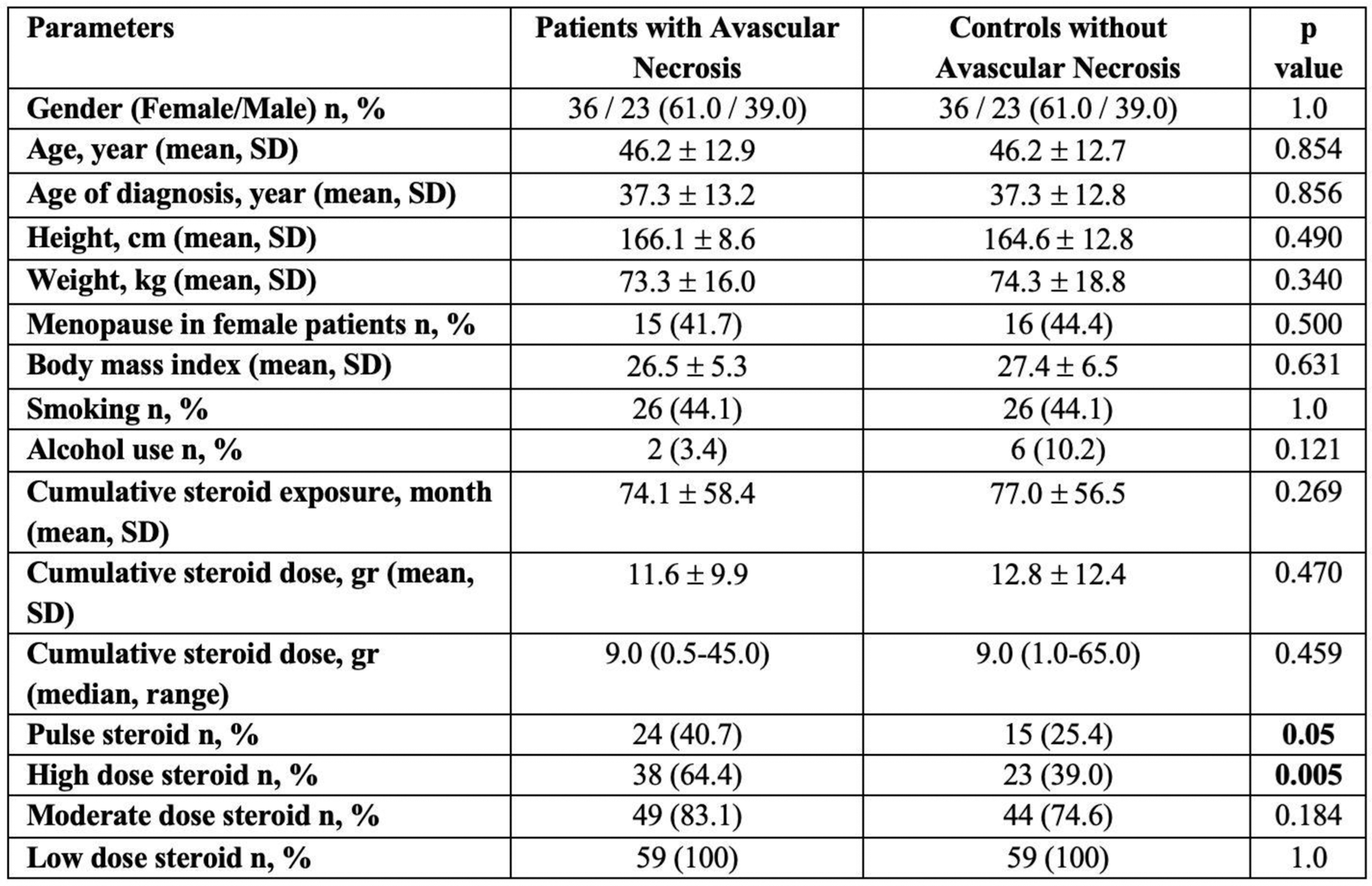
Results: A total of 1400 RA, 610 Behçet’s disease (BD), 600 SLE, 110 systemic sclerosis (SSc), 650 familial Mediterranean fever (FMF), 100 ANCA-associated vasculitis (AAV), 60 adult-onset Still’s disease (AOSD), 50 Takayasu arteritis (TAK), 45 IgA vasculitis (IgAV), 22 IgG4-related disease (IgG4 RD), and 4 chronic recurrent nonbacterial osteomyelitis (CRMO) patients were screened. Demographic and clinical characteristics were similar between the AVN and control groups. The AVN group included 13 RA, 9 SLE, 17 BD, 1 gout, 1 sarcoidosis, 5 AAV, 2 IgAV, 1 AOSD, 3 SSc, 3 IgG4 RD, 2 FMF, 1 CRMO, and 1 TAK, with matched controls. AVN affected one site in 23 patients, two sites in 28, three sites in 6, and four sites in 2 patients. The left hip (37), right hip (35), right knee (17), and left knee (10) were the most common sites, with less frequent involvement of shoulders, wrists, and foot joints. Bone mineral density was normal in 10%, osteopenic in 20%, and osteoporotic in 70%. Calcium supplementation before AVN was regular in 37.5%, irregular in 15.3%, and absent in 47.4%. Regular asetlsalicyclic acid (ASA) use was noted in 22% and irregular in 5.1%. High-dose (64.4% vs. 39.0%, p=0.005) and pulse steroid use (40.7% vs. 25.4%, p=0.05) were significantly more frequent in the AVN group, while cumulative steroid dose was similar (11.6±9.9 g vs. 12.8±12.4 g, p=0.470). Methotrexate, hydroxychloroquine, leflunomide, TNF inhibitors, tocilizumab, rituximab, IVIg, JAK inhibitors, colchicine, cyclophosphamide, mycophenolate mofetil, and calcineurin inhibitors were used similarly in both groups. Among AVN patients, 10.2% underwent core decompression, 20.3% joint replacement surgery, 25.4% hyperbaric oxygen therapy, and 93.2% had steroid reduction or discontinuation. Additionally, 20.2% received ASA for joint perfusion.
Conclusion: This study highlights the significant association between high-dose and pulse CS use and the development of AVN in patients with rheumatologic diseases. Despite similar cumulative steroid doses, AVN patients exhibited more frequent and severe joint involvement, particularly in the hips and knees. Management strategies, including surgical interventions such as core decompression and joint replacement, alongside weight-bearing restrictions and CS tapering, were critical for optimizing patient outcomes. These findings emphasize the need for careful CS management, regular bone health monitoring, and early identification of high-risk patients to prevent AVN-related complications.
REFERENCES: NIL.
Table 1 . Demographic and clinical characteristics of avascular necrosis and matched-disease control group without avascular necrosis.
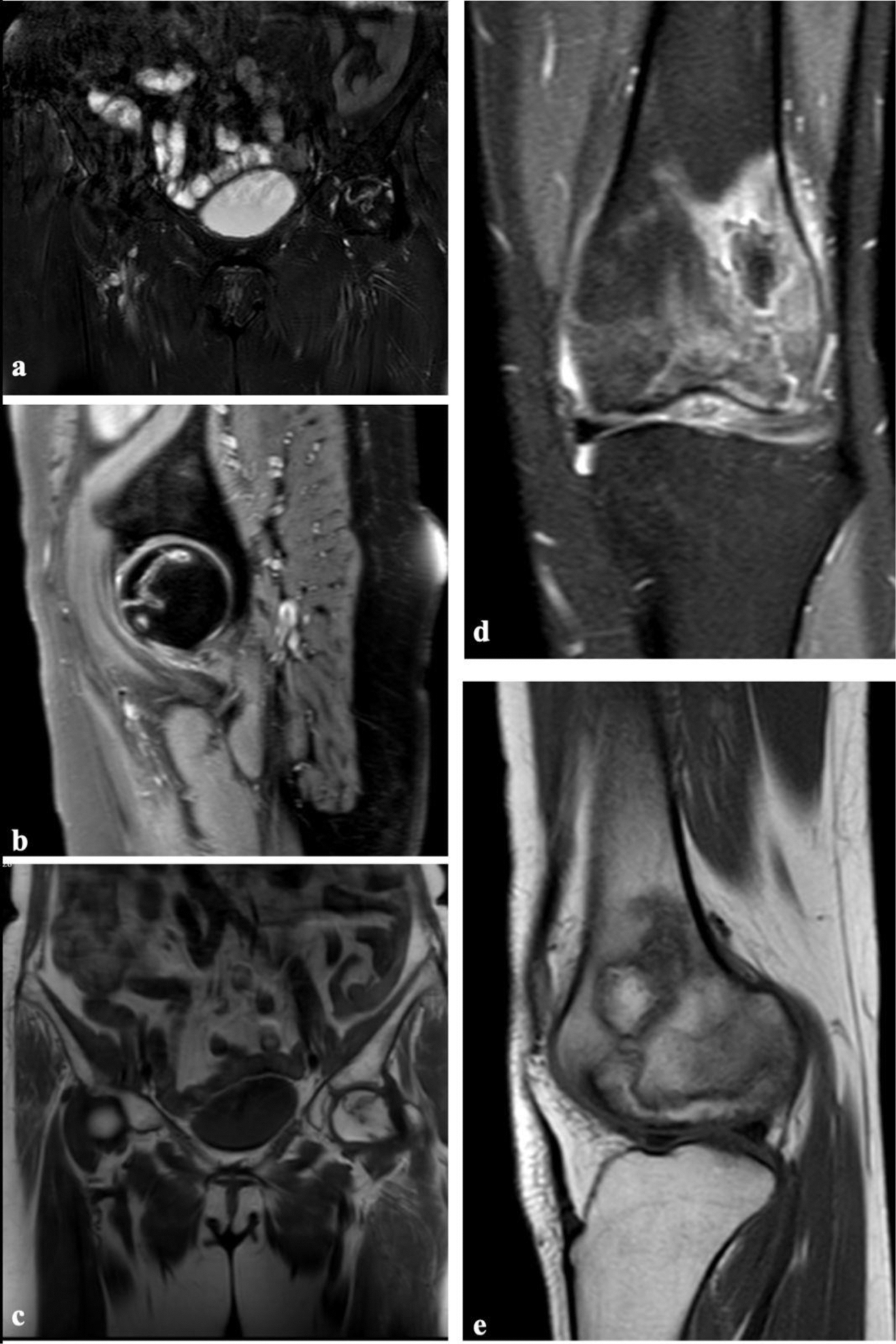
Examples of Avascular Necrosis on Magnetic Resonance Imaging Figure 1a, b, and c demonstrate an example of hip avascular necrosis (AVN) in coronal fat-suppressed T2-weighted sequence (a), sagittal fat-suppressed T2-weighted sequence (b), and coronal T1-weighted sequence (c), showing geographic signal changes in the femoral head while preserving the femoral contour and acetabulum. Figure 1d and e present an example of AVN in the left femur, shown in coronal fat-suppressed T2-weighted sequence (d) and sagittal T1-weighted sequence (e), displaying geographic signal changes and significant edema in the distal metaphyseal-diaphyseal region of the left femur.
Acknowledgements: Nil.
Disclosure of Interests: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (