fetching data ... 
Background: Patients with rheumatoid arthritis (RA) are predisposed to several potentially serious respiratory diseases, such as interstitial lung disease (ILD) and obstructive lung disease. Pulmonary function tests are practical and accessible first-line tools to diagnose and monitor respiratory diseases. Traditionally, pulmonary function tests have been presented as absolute values and percentages of predicted values for the individual patient (% predicted), with values below 80% of predicted commonly classified as “reduced lung function”. Obstructive ventilatory impairment can be assessed by the forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) (FEV1/FVC) ratio, with a ratio below 0.7 widely used to define abnormal values. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) advocates the use of the fixed FEV1/FVC ratio for defining obstruction because of its simplicity and independence from reference equations [1]. However, these approaches may lead to overdiagnosis, particularly in older adults, as these thresholds fail to account for the natural variability and age-related changes in lung function [2]. The European Respiratory Society (ERS) and Global Lung Function Initiative (GLI) therefore advocate for use of Z-scores, which better account for the natural variability in age, sex, height and ethnicity, and define the lower limit of normal (LLN) as a Z-score of -1.645 [3]. Although Z-scores offer advantages like reducing misclassifications, many clinicians and researchers continue to rely on the 80% predicted cut-off and fixed FEV1/FVC ratio thresholds.
Objectives: To evaluate different lung function cut-off criteria in RA patients by comparing the 80% predicted cut-off and the fixed FEV1/FVC ratio of 0.7 with the Z-score approach, focusing on how these criteria may lead to differences in patient classification.
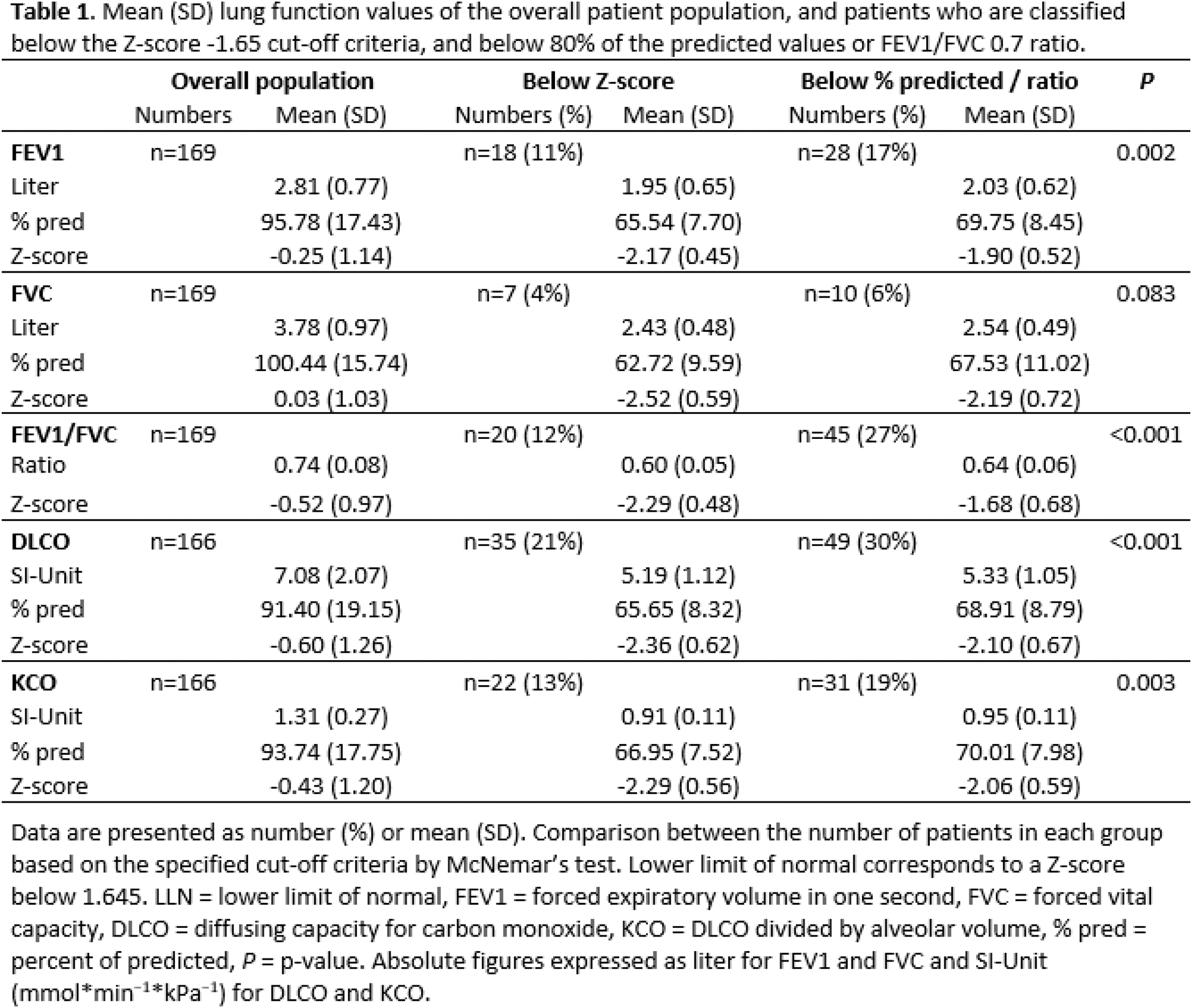
Methods: We analyzed pulmonary function tests from RA patients participating in the nationwide multicenter ARCTIC-FORWARD study, a 10-year follow up of the ARCTIC trial [4]. Pulmonary function variables included FEV1, FVC, the FEV1/FVC ratio, diffusing capacity for carbon monoxide (DLCO), and DLCO divided by alveolar volume (KCO). Both percentage of predicted values and Z-scores were calculated using GLI-2012 and -2017 reference values. Reduced lung function was defined according to three definitions: values below 80% predicted, FEV1/FVC ratio below 0.7, or values below LLN (Z-score below -1.645). Pulmonary-related comorbidities were self-reported by the patient. McNemar’s test was used to compare the number of patients in each group based on the specified cut-off criteria.
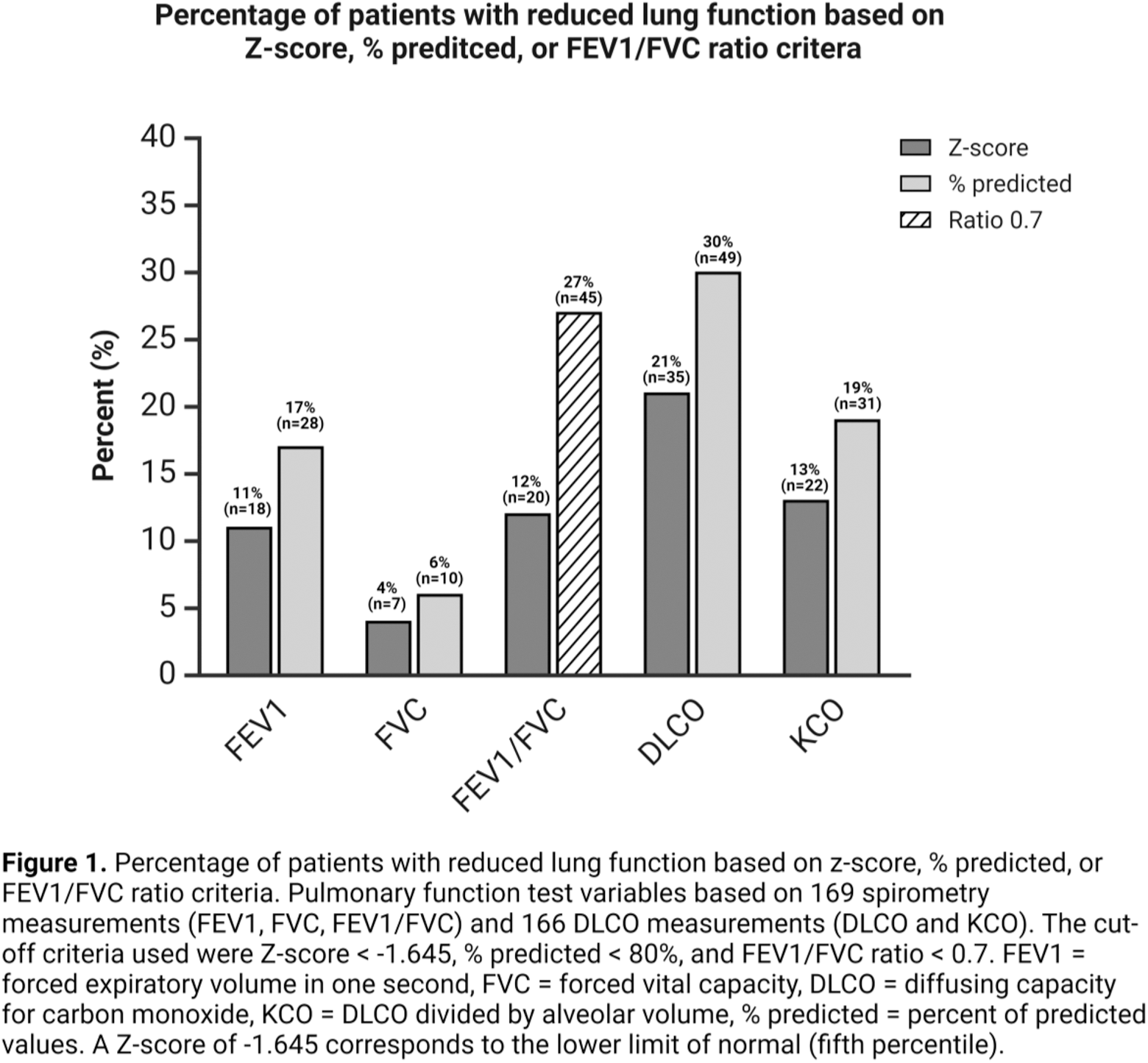
Results: A total of 179 RA patients were included in the study, with pulmonary function tests available from 169 patients (169 spirometry and 166 DLCO measurements). Among these patients, 107 (63%) were female. The mean (standard deviation, SD) age was 61.3 (13.1) years, height was 170.9 (9.3) cm, weight was 78.7 (18.0) kg, and BMI was 26.8 (5.3) kg/m 2 . Thirteen patients (7%) reported asthma, 10 patients (6%) reported known chronic obstructive pulmonary disease, and two patients (1%) reported known ILD. A higher proportion of patients were classified as abnormal according to the 80% predicted cut-off compared to the Z-score cut-off across all parameters (Figure 1). The most notable discrepancy was in the FEV1/FVC ratio; with 27% (n=45) of patients classified as obstructive based on ratio < 0.7, compared to 12% (n=20) using the Z-score criteria (Table 1). Similar differences were found for DLCO, with 30% (n=49) of patients having values below 80% of the predicted, compared to 21% (n=35) of patients below the Z-score criteria. A six-percentage point difference was observed for both FEV1 and KCO. When assessing patients using the percentage of predicted and the FEV1/FVC ratio of 0.7 criteria, 49% of patients (82 of 169) had at least one abnormal measurement—such as FEV1, FVC, FEV1/FVC (ratio < 0.7), DLCO, or KCO below 80% of the predicted value. In comparison, the Z-score criteria identified 33% of patients (55 out of 169) with similar abnormalities.
Conclusion: A higher proportion of patients with RA were classified as having reduced lung function when using percentage of predicted values and the fixed FEV1/FVC ratio <0.7, compared to the Z-score criteria. This highlights the potential for overdiagnosis when relying solely on percentage of predicted values. In the context of screening and diagnosis, adopting Z-scores could provide a more individualized assessment of lung function in patients with RA, potentially enhancing diagnostic precision and promoting efficient use of healthcare resources, thereby reducing the risk of unnecessary evaluations and treatments.
REFERENCES: [1] Agustí, A., et al., Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J, 2023. 61 (4).
[2] Miller, M.R., et al., Interpreting lung function data using 80% predicted and fixed thresholds misclassifies more than 20% of patients. Chest, 2011. 139 (1): p. 52-9.
[3] Stanojevic, S., et al., ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J, 2021.
[4] Haavardsholm, E.A., et al., Ultrasound in management of rheumatoid arthritis: ARCTIC randomised controlled strategy trial. Bmj, 2016. 354 : p. i4205.
Acknowledgements: NIL.
Disclosure of Interests: Henrik Mangseth: None declared, Eirik Ikdahl: None declared, Michael T Durheim AstraZeneca and Pfizer, Boehringer Ingelheim and Roche, Gina Brinkmann: None declared, Nina Paulshus Sundlisæter: None declared, Joe Sexton: None declared, Morten Sand: None declared, Anna-Birgitte Aga Abbvie, Lilly, Novartis, and Pfizer, Espen A. Haavardsholm AbbVie, Eli Lilly, Novartis and Pfizer, Siri Lillegraven: None declared, Lena B Norberg: None declared.
© The Authors 2025. This abstract is an open access article published in Annals of Rheumatic Diseases under the CC BY-NC-ND license (